

Pain in Oncology, Reality and Paradox of Homeopathic Care
BAGOT Jean-Lionel 1, 2, 3, *![]()
- Main General Practice Surgery, 5, Place des Halles, 67000 Strasbourg, France
- Robertsau Radiotherapy Centre, 184 route de la Wantzenau, 67000 Strasbourg, France
- Saint-Vincent Hospital Group, Department of Integrative Medicine, Saint Anne Hospital, rue Philippe Thys, 67000 Strasbourg, France
* Correspondence: BAGOT Jean-Lionel![]()
Received: May 31, 2018 | Accepted: August 30, 2018 | Published: September 17, 2018
OBM Integrative and Complementary Medicine 2018, Volume 3, Issue 3 doi:10.21926/obm.icm.1803019
Academic Editor: Michael Frass
Special Issue: Application of Homeopathy in Oncology Patients
Recommended citation: Bagot JL. Pain in Oncology, Reality and Paradox of Homeopathic Care. OBM Integrative and Complementary Medicine 2018;3(3):019; doi:10.21926/obm.icm.1803019.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
Background: After fatigue, pain is one of the major complaints from cancer patients. Regular use of Class 1 analgesics may cause side effects and is not always sufficient to relieve pain. Homeopathy is the complementary and integrative medicine most frequently used in France in supportive care in oncology (SCO). What is its place in the treatment of pain? Method: Extraction and analysis of results concerning pain from three surveys, two of which were carried out in France, on the main indications of homeopathy in SCO from doctors specialising in oncology (DSO), non-homeopathic general practitioners (NHGP) and homeopathic general practitioners (HGP), and the third being among patients in a cancer ward in Vienna. Results: Both NHGP and DSO are interested in homeopathic therapy primarily for the pain of chemo-induced peripheral neuropathy (CIPN) but also for musculoskeletal pain. Compared to a control group, patients treated with homeopathy experienced more pain relief (p <0.001). Paradoxically, the HGPs place the relevance of homeopathic treatment of pain only in twelfth place. Conclusion: This work should encourage homeopathic physicians to reinvest in pain management, particularly that of CIPNs. The systematic evaluation of pain on the visual analogue scale (VAS) at each consultation, and a good knowledge of the physiopathological mechanisms involved, should help restore their confidence. The homeopathic prescription can be proposed from the recommendations of the International Homeopathic Society of Supportive Care in Oncology (IHSSCO) or, in more difficult cases, after an individualised consultation and répertorisation following the principles of similarity and globality of symptoms.
Keywords
Chemotherapy induced peripheral neuropathy; homeopathy; integrative oncology; musculoskeletal disorders; pain, supportive care
1. Introduction
Subsequent only to fatigue and sleep disorders, pain is the third complaint expressed by patients being treated for cancer, according to Cleeland et al. [1]. Class 1 analgesics are very frequently prescribed and consumed for this complaint. Their regular usage by oncology patients is often problematic due to their potential side effects [2].
As the integrative and complementary medicine most used in supportive care in oncology (SCO) in France [3,4], homeopathy prescribed to patients being treated for cancer significantly reduced pain (p <0.001) compared with the control group receiving only conventional analgesics [5].
As a specialist in supportive care in oncology, I frequently use homeopathic medicine for this indication. With nearly 4000 support consultations per year [6], the positive feedback of patients confirms the strong medical benefit of homeopathy for pain management.
To further investigate the role of homeopathy, I have studied and compared the results of two surveys conducted in France as well as one survey among patients in a cancer ward in Vienna [5], on the helpfulness of homeopathy in SCO by combining the results of these different studies with my personal experience as a clinician, I sought to discover what concrete suggestions can be made concerning homeopathic analgesic prescriptions for SCO.
2. Important Note
I will speak here only of the pain caused by cancer treatments. The pain related to the cancer itself and its development most often require level 2 or 3 analgesics.
3. Results Concerning the Homeopathic Management of Pain
I had the opportunity to analyse two surveys regarding homeopathic SCO by French physicians: 150 medical specialists in oncology (radiotherapists, oncologists, and haematologists), 100 general practitioners without training in homeopathy, and 97 general practitioner homeopaths. I then extracted from these surveys the data concerning the management of pain. My involvement with the research that supports this article followed a decision made in concertation with the homeopathic product manufacturer Boiron Laboratories to undertake the surveys. Boiron commissioned the survey research from two independent healthcare market research agencies, Axess Research and AplusA. The statistical analysis of the results was carried out by these agencies and I made my own analysis and interpretations of the outcomes concerning the management of pain by homeopathy in SCO because they raise questions which we will discuss here.
4. For Physicians Specializing in Oncology
Chemotherapy-induced peripheral neuropathy is manifested mainly by paraesthesia and pain in the extremities of hands and feet, such as tingling or stinging, aggravated by exposure to cold and pressure. They represent the fifth complaint for all cancers and the second in colon cancer due to the therapeutic use of oxaliplatin [1]. Among the various symptoms addressed, the treatment of peripheral neuropathies especially poses a problem for specialists in oncology that were questioned in the first study. Eighty percent of physicians are dissatisfied with currently available conventional treatments and 78% are interested in a homeopathic therapy for this indication.
Musculoskeletal pain (MSP) occurs mainly after anti-aromatase therapy. In this indication, 39% of cancer specialists say they are not satisfied with the available conventional treatments and 67% are interested in homeopathic treatment.
5. For Non-homeopathic General Practitioners (NHGP)
Frequently, pain is the reason for NHGP consultation as it ranks, in these two surveys, among23 symptoms studied, just after fatigue and before anxiety.
NHGPs, like oncologists, are dissatisfied with the conventional treatments available for peripheral neuropathic pain and rank this indication as being the most potential for homeopathic treatment in SCO.
With regards to musculoskeletal pain, the degree of satisfaction for the available conventional treatments is only moderate. However, the use of homeopathy seems to them to be less judicious for this type of pain.
6. For Homeopathic GPs (HGP)
Differing from their non-homeopathic colleagues, pain ranks sixth among symptoms addressed during consultations. Regarding their opinion on the relevance of homeopathic treatment of pain, they ranked it in twelfth position with a score of 6.1 / 10. Peripheral neuropathies are not ranked any better as they give the relevance of homeopathy in this indication a score of 5.8 / 10.
Musculoskeletal pain is a slightly more frequent reason for consultation with a score of 6.6 / 10 and a better potential with 6.6 / 10. The HGPs only rank them in 10th position for homeopathic indications in SCO.
7. For Patients
The Michael Frass et al. study shows that by improving the overall condition and quality of life of patients with individualized homeopathic treatment, it significantly improves many other symptoms, including pain. (Table 1).
Table 1 (with the permission of the author): Comparison of first vs. third visit with adjunctive homeopathy.

8. Discussion and Suggestions
Pain is an analyzed via semiotics in homeopathy as it is an eminently personal and subjective symptom. It provides the homeopathic doctor with valuable information for choosing the homeopathic medicine best suited to their patient. With nearly thousands of different varieties of pain sensations described in the original James Tylor Kent repertory [7], pain is certainly the most studied symptom in homeopathy. In addition to its semiological interest for the homeopathic physician, the study by Michael Frass et al. suggests the effectiveness of its prescription in SCO for the treatment of pain.
However, the results of the two studies involving doctors challenges us because it brings out an interesting paradox:
-
On the one hand, oncologists and NHGPs have a high expectation for the homeopathic treatment of pain, a symptom for which these professionals feel relatively powerless to address in SCO.
-
On the other hand, surprisingly, HGPs are only moderately confident in the pain management of patients, whether measured by the frequency of pain mentioned during consultation, or by the relevance of the homeopathic treatment.
9. How Can We Explain this Difference of Perception?
The first explanation is the absence of exact quantification of pain during general practitioner consultations. From one consultation to another, pain is always present and challenges the doctor. However, the previous treatment may have reduced the intensity and frequency of pain. The lack of precise quantification does not make it possible to evaluate the real effectiveness of the prescribed treatment and the degree of relief the patient experiences. The complaint remains the same, even when pain has reduced.
This repeated complaint can disturb the doctor's assessment of the effectiveness of the therapy. It should be recalled here that a reduction of two points on the visual analogue scale (VAS) of pain is sufficient for a conventional analgesic medicine to be considered effective in the treatment of pain.
We strongly encourage GPs and especially homeopaths to mention in their clinical observations the pain VAS of patients, obtained either with a ruler or analogically by simply asking the question: “From zero to 10, how much do you evaluate your pain: zero being the absence of pain, 10 being the maximum pain imaginable?” Monitoring the pain via the VAS curve gives the caregiver a clearer analysis of the clinical situation and the activity of the current treatment. The simple question: “Are you still in pain?” risks receiving a positive answer as long as cancer treatments responsible for the pain are ongoing. Discouraged, the doctor no longer asks the question, thus perhaps explaining the low frequency of the complaint of "pain" found in the questionnaire from HGPs.
A second possibility is the sometimes difficult choice of the best homeopathic medicine. This requires noticing all the homeopathic semiology and drawing a listing made complicated by the multiplicity of symptoms present during SCO. Faced with these difficulties, it might be useful to reflect on the physiopathology of this pain. Looking for the aetiology, also called causality, gives us valuable indications in the choice of homeopathic treatment [8].
The homeopathic physician should not confuse the pain associated with the cancerous disease itself and the pain related to the side effects of cancer treatments. In the first case, the homeopathic prescription will indeed be insufficient. Level III analgesics are necessary and effective.
10. Musculoskeletal Pain (MSP)
We can't help but take note of the hepatic, nephrological, or cardiac disturbances sometimes caused by regular use of class 1 analgesics in our consultations. A recent meta-analysis [9] concludes that there is no convincing evidence of paracetamol being different from placebo with regards to quality of life, use of rescue medication, or patient satisfaction or preference among cancer patients. Is it not possible that homeopathy could be an additional therapy available to the oncologist or supportive care physician in the management of pain and thus help to reduce iatrogenic risks?
Evaluation of the homeopathic management of MSP was carried out in the EPI3 pharmacoepidemiology study [10]. Of 1153 patients followed for one year by 825 GPs belonging to three different categories (one-third NHGPs, one-third mixed GPs, and one-third HGPs), the clinical benefits and evolution of musculoskeletal pain were compared in the three groups. Notably, patients treated by HGPs reported that they consumed 50% less nonsteroidal anti-inflammatory drugs and 25% fewer analgesics than those followed by NHGPs for chronic musculoskeletal pain. The authors note that this significant difference in chemical medication consumption was achieved without lessening efficacy and without loss of therapeutic opportunity over the 12 months of the follow-up.
In SCO, the most common reason for consultation for chronic MSP is pain secondary to taking anti-aromatase. This hormone-privation is prescribed as adjunctive therapy for hormone-sensitive breast cancer in menopausal women. When pain appears, it persists for as long as there is induced oestrogen deficiency, which is to say during the five to ten years of treatment. Homeopathy may sometimes appear to be insufficient to the prescribing physician, yet, when asked, patients are satisfied and come back regularly to continue the treatment of homeopathic support. The preliminary open study conducted in 2016 by Jean-Claude Karp et al. confirms the indication for homeopathic treatment in this situation [11]. It compared 20 patients starting anti-aromatase treatment with 20 patients starting the same treatment in combination with Ruta graveolens 5C and Rhus toxicodendron 9C, at 5 pellets each morning and evening for 3 months. A statistically significant decrease in joint pain occurred in the group treated with homeopathy (p = 0.0001). These positive preliminary results will make it possible to conduct studies on a larger number of patients. They should encourage homeopathic physicians to trust in the analgesic activity of these medicines.
In 2016, a learned society, the International Homeopathic Society for Supportive Care in Oncology (IHSSCO), was created to facilitate and develop the practice, teaching, research, and promotion of homeopathic therapy in the context of supportive care in oncology [12]. It recommended the same protocol developed by a consensus of experts published in 2017 [13], but modified it by decreasing the number of pellets taken at a time to facilitate compliance. It suggests the following for treatment of musculoskeletal pain: Rhus toxicodendron 9C and Ruta graveolens 5C, 3 pellets of each to dissolve in the mouth together morning, noon, and evening.
In our experience, if we want the analgesic action to persist beyond 3 months, it is necessary to treat the patient's terrain with a constitutional medication prescribed according to the principle of similarity and globality of symptoms. From the physiopathological point of view, it must be assumed that oestrogen deficiency is responsible for these joint symptoms. These joint pains especially affect the extremities (feet and hands) and they are ankylosis-type pain, improved by movement and aggravated upon waking. If these symptoms first make us think of Rhus toxicodendron, the analysis also presents Sepia officinalis (Figure 1). Apart from the pain, the patients often express other symptoms such as low morale, low libido, cutaneous and vaginal dryness, and repeated urinary infections, all of which confirm the indication of Sepia officinalis, the homeopathic medicine specific to oestrogen deficiency.
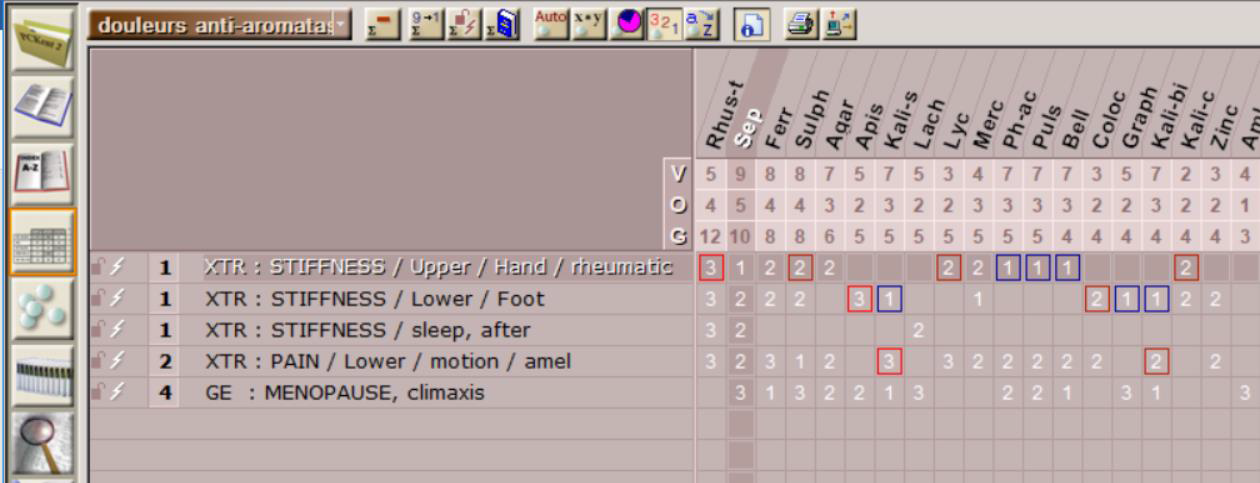
Figure 1 Repertory MSP secondary to antiaromatases on PCKent 2.2®. V=value, O=occurrence, G=Grade, XTR=extremity. GE=generality, Rhus-t=Rhus toxicodendron, Sep=Sepia officinalis, Ferr=Ferrum metallicum, Sulph=Sulphur, Agar=Agaricus muscarinus, Apis=Apis mellifica, Kali-s=Kalium sulphuricum, Lach=Lachesis mutus, Lyc=Lycopodium clavatum, Merc=Mercurius solubilis, Ph-ac=Phosphoricum acidum
The chronic and persistent nature of the pain, its aggravation by wet cold, and its iatrogenic origin indicate a sycotic reaction mode that can be treated if necessary with medicines like Thuya occidentalis, Natrum sulfuricum, and/or Medorrhinum.
Deformity of the hand joints and a previous history of radiotherapy may point towards the luetic reaction mode and lead to prescribing Radium bromatum, whose modes of improvement by movement and hot applications are the same as that of Rhus toxicodendron.
Other lesser-known local action medicines are: Caulophyllum thalictroides for intermittent and paroxysmal pain of the small hand and foot joints with articular stiffness or Actaea spicata for deformities and painful swelling of the first phalanges, which tend to be very sensitive to touch, but the pain is aggravated by movement. For the sake of completeness, Polyganum aviculare for pain in the second phalange of the fingers can also be used [14].
11. Chemo-induced Peripheral Neuropathies (CIPN)
With an incidence of 30–70%, CIPN is the second limiting factor for chemotherapy after haematological toxicity [15]. In 30% of cases, the improvement is incomplete after discontinuation of chemotherapy, making neuropathic pain a frequent reason for consultation in SCO.
CIPNs are mainly expressed by stinging pain and tingling of the hands and feet. The main agents responsible for peripheral neuropathies are platinum salts, taxanes such as paclitaxel and docetaxel, vinca alkaloids bound to a monoclonal antibody, and bortezomib [16]. No neuroprotective treatment exists [17]. The only recommended preventive treatment is calcium and magnesium infusion prior to oxaliplatin [18]. There are no official recommendations for preventive treatment for other chemotherapies. Only dose reduction and spacing or discontinuation of chemotherapy are advised. Once established, the CIPNs are often resistant to conventional analgesics. This probably explains the high degree of dissatisfaction of oncologists and NHGPs and their significant demand for homeopathic management of these symptoms. Yet, homeopathic doctors are once again the least optimistic about the value of their treatment for this indication.
Our clinical experience shows that homeopathic treatment is especially effective in prevention at the beginning of the symptoms rather than in the treatment of well-established neuropathies. Therefore, it is important to anticipate the symptoms in homeopathic SCO and to start accompanying treatments from the first chemotherapy sessions.
The IHSSCO, in its recommendations by a professional consensus, proposes the following in prevention of peripheral neuropathies:
- Nerves 8D or 4C, 1 ampoule in a little water, to keep a short time in the mouth before swallowing, morning and evening on D-1, D-0, D-1, D-2 and longer if tingling persists.
- Phosphorus 15C, 3 pellets in the evening on D-1, D-0, D-1, and D-2.
- Oxalicum acidum 9C, 3 pellets in the morning on D-1, D-0, D-1, and D-2 of associated oxaliplatin treatment.
From our experience and that of many of our colleagues, Hypericum perforatum is not very effective in the homeopathic treatment of CIPN pain. Although the physiopathological mechanisms responsible for iatrogenic neuropathies are still unclear, we are certain that they are not of traumatic origin, a major aetiological indication of Hypericum perforatum. Its frequent and automatic prescription by some colleagues may explain their therapeutic disappointments.
We carried out an online inventory for didactic purposes, looking for the most appropriate medication. Only the drugs present in the aetiological category "inflammation of the nerves" were selected. We identified the main symptoms described in the DN4 assessment questionnaire [19]. This theoretical exercise allowed us to identify five candidate medicines: Natrum muriaticum, Phosphorus, Arsenicum album, Sulfur, and Aconitum napellus from which we can choose according to the modalities and characteristics specific to each patient; this principle of individualization is necessary in homeopathy. We found that Hypericum perforatum only appears in 17th position.
The disruption of sodium, potassium, and calcium exchanges in the ion channels of the axonal membranes by chemotherapy (oxaliplatin in particular), is one of the mechanisms responsible for CIPNs. Natrum muriaticum soothes neuropathic pain and is at the top of the list of suggested medicines likely due to its ability to regulate cellular ion exchange at the sodium pump (Figure 2).
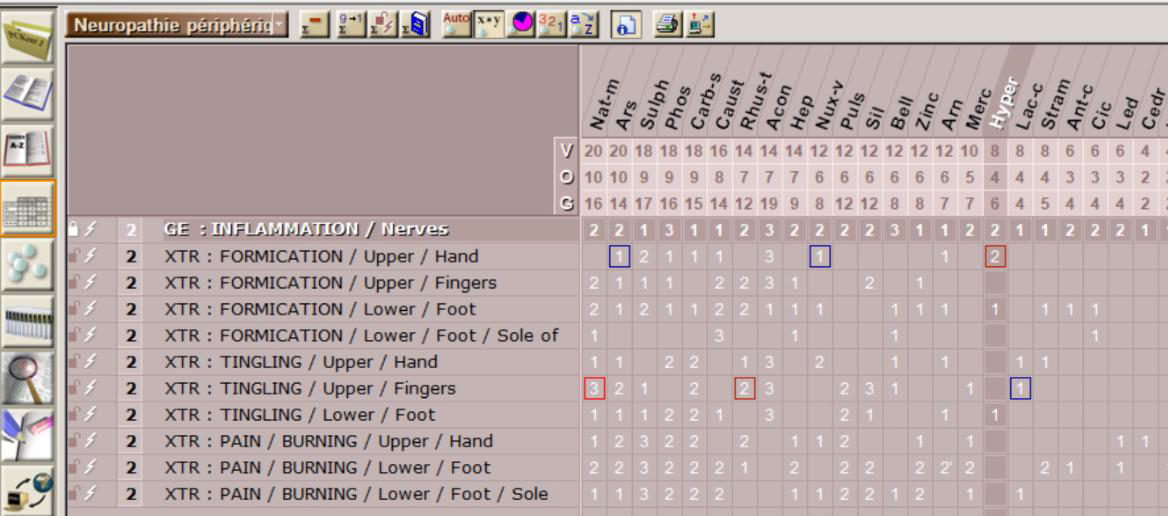
Figure 2 Repertory of painful symptoms of peripheral neuropathies according to DN4 questionnaire on PCKent 2.2®. V=value, O=occurrence, G=Grade, GE=generality, XTR=extremity, Nat-m=Natrum muriaticum, Ars=Arsenicum album, Sulph=Sulfur, Phos=Phosphorus, Carb-s=Carboneum sulphuratum, Caust=Causticum, Hyper=Hypericum
Another mechanism exhibited in the pathophysiology of CIPN is the inflammation of the spinal ganglia by a high presence of pro-inflammatory cytokines (IL1, IL6, and TNF-alpha) [20]. During chemotherapy, immune cells and cancer cells induce pro-inflammatory cytokines around nerve endings [21]. Phosphorus has been shown to exert an inhibitory effect in vitro on neutrophilic granulocytes. These play a fundamental role in acute inflammation, even at very high dilutions (10 -15) [22].
The anti-inflammatory action of Phosphorus (as described in the homeopathic literature) both on the peripheral nervous tissue and on the central nervous system can explain its clinical activity, which I personally observed in the control of peripheral neuropathies. IHSSCO routinely advises this medication preventively the day before, on the day of, and the day after each chemotherapy. It can also be used in the case of painful sequelae.
When painful manifestations are persistent, the aggravation modalities will be important to consider for the choice of treatment:
- For aggravation by cold we have two medicine choices. Arsenicum album is indicated in progressive bilateral, ascending sensory and motor paralysis of the hands and feet, which is preceded by numbness and tingling. The extremities are cold and the osteotendinous reflexes are diminished or even abolished. The musculature weakens and cramps are frequent, especially at night in bed. Aconitum napellus is indicated in neuropathic pain of recent appearance in conjunction with paraesthesia, frequently experienced as a tingling sensation then numbness after exposure to cold.
- For aggravation by heat, Sulfur helps when there is burning foot pain, aggravated by wearing shoes and relieved by walking barefoot on floor tiles or getting out of bed at night. This clinical situation occurs especially when neuropathies become chronic.
In fact, in the end, the choice of the correct remedy for the given indication depends on the overall picture the patient is presenting.
Organotherapy is a diluted and dynamized preparation of rabbit or pork organ extracts. It is used to restore and support the proper functioning of the patient's corresponding organ. Organotherapy is a supplement to homeopathic treatment to strengthen its action. The indication of the organotheray strain Nerves, is intriguing to us considering the pathophysiology of the neurological post-chemotherapy syndrome. Low organotherapy dilutions (4C) stimulate and high dilutions (30C) slow down the activity of the organ of the same name. This is why IHSSCO recommends Nerves 8D or 4C one to three times a day in the prevention and treatment of chemically-induced neuropathies. Given the very positive feedback of patients, some French oncologists have made it a routine prescription in neuropathies.
12. Conclusion
Pain is a very common side effect, and it often requires the use of class 1 analgesics whose relative effectiveness and potential toxicity make a regular prescription problematic. Homeopathic therapy with its medicinal status provides a guarantee of safety and the assurance of a prescription by a qualified doctor (in France). Considered relevant by oncologists as well as by NHGPs, homeopathic pain management represents a possible alternative to class 1 analgesics and anti-inflammatories. This work should encourage homeopathic physicians to re-evaluate pain management by utilizing the VAS at each consultation as well as discerning the pathophysiological mechanisms responsible for pain for the best-suited choice of their medicines. If the study and the listing of the totality of the symptoms is necessary for an individual prescription, the recommendations of the IHSSCO will be useful. Clinical studies evaluating the actual benefit of homeopathy in the management of pain secondary to cancer treatments are to be encouraged.
Acknowledgements
The author would like to thank Aurore Serral and Catherine Girotti from Laboratoires Boiron for giving him access to and presenting the first two studies. My thanks also go to the consulting firms AplusA and Axess Research for reviewing and validating the results concerning their respective work and to Michael Frass for letting me have and publish the complete table of the results of his study.
Author Contributions
The author did all works.
Competing Interests
The author state that he participates in occasional interventions (expert reports, conferences, advisory and training activities) for Laboratoires BOIRON.
References
- Cleeland CS, Zhao F, Chang VT, Sloan JA, O'Mara AM, Gilman PB, et al. The symptom burden of cancer: evidence for a core set of cancer-related and treatment-related symptoms from the Eastern Cooperative Oncology Group Symptom Outcomes and Practice Patterns study. Cancer. 2013; 119: 4333-4340. [CrossRef]
- Roberts E, Delgado Nunes V, Buckner S, LatchemS, Constanti M, Miller P, et al. Paracetamol: not as safe as we thought? A systematic literature review of observational studies. Ann Rheum Dis. 2016; 75: 552-559. [CrossRef]
- Rodrigues M. Use of alternative and complementary medicines by cancer patients. Results of the MAC-AERIO EUROCANCER 2010 study [Utilisation des médecines alternatives et complémentaires par les patients en cancérologie: résultats de l’étude MAC-AERIO EUROCANCER 2010.]. John Libbey Eurotext, Paris 2010, pp. 95-96.
- Legrand A. Etude de la prévalence de l’utilisation des médecines complémentaires par les patients atteints de cancer. A partir de 535 questionnaires recueillis d’avril à juin 2017 à Strasbourg [Thèse de doctorat de médecine] Université de Strasbourg. Faculté de Médecine, 2018, n10.
- Frass M, Friehs H, Thallinger C et al. Influence of adjunctive classical homeopathy on global health status and subjective wellbeing in cancer patients - A pragmatic randomized controlled trial. Complement Ther Med. 2015; 23: 309-317. [CrossRef]
- Bagot JL. Cancer & homeopathy, how to alleviate the side effects of chemotherapy, radiation, surgery and hormone therapy. Narayana (Ed), Unimedica Publisher, Kandern, Germany, 2014, pp1-330.
- Kent JT. Repertory of the homeopathic materia medica, 4 ed. Chicago: Ehrhart & Karl; 1935.
- Bagot JL. The specific characteristics of a homeopathic consultation. Revhom. 2018; 9: e17-e22.
- Wiffen PJ, Derry S, Moore R, McNicol ED, Bell RF, Carr DB et al. Oral paracetamol (acetaminophen) for cancer pain. Cochrane Database of Systematic Reviews. 2017. Art. No.: CD012637.
- Rossignol M, Begaud B, Engel P, Avouac B, Lert F, Rouillon F et al. Impact of physician preferences for homeopathic or conventional medicines on patients with musculoskeletal disorders: Results from the EPI3-MSD cohort. Pharmacoepidemiol Drug Saf. 2012; 21: 1093-1101. [CrossRef]
- Karp JC, Sanchez C, Guilbert P, Mina W, Demonceaux A, Curé H. Treatment with Ruta graveolens 5CH and Rhus toxicodendron 9CH may reduce joint pain and stiffness linked to aromatase inhibitors in women with early breast cancer: results of a pilot observational study. Homeopathy. 2016; 105: 299-308. [CrossRef]
- Bagot JL. Création de la société homéopathique internationale de soins de support en oncologie (SHISSO). Revhom. 2017; 8: 93-94.
- Bagot JL, Karp JC, Messerschmitt C, Lavallée V, Blajman H, Veron F et al. Therapeutic recommendations of the International Homeopathic Society of Supportive Care in Oncology (IHSSC0). Revhom 2017; 8: e47-e55.
- Voisin H. Repertory for the homeopathic practitioner narayana (Ed), Kandern, Germany, 2019, pp1-1300 (In press).
- Andersen KG, Kehlet H. Persistent pain after breast cancer treatment: a critical review of risk factors and strategies for prevention. J Pain Off J Am Pain Soc. 2011; 12: 725-746. [CrossRef]
- Miltenburg NC, Boogerd W. Chemotherapy-induced neuropathy: A comprehensive survey. Cancer Treat Rev. 2014; 40: 872-882. [CrossRef]
- Verstappen CC, Heimans JJ, Hoekman K, Postma TJ. Neurotoxic complications of chemotherapy in patients with cancer: clinical signs and optimal management. Drugs. 2003; 63: 1549-1563. [CrossRef]
- AFSOS. Fiches referentiels neuropathie périphérique et cancer. Available from : http://www.afsos.org/fiche-referentiel/neuropathie-peripherique-cancer/
- Bouhassira D, Attal N, Fermanian J, Alchaar H, Gautron M, Masquelier E et al. Development and validation of the neuropathic pain symptom inventory. Pain. 2004; 108: 248-257. [CrossRef]
- Wang XM, Lehky TJ, Brell JM, Dorsey SG. Discovering cytokines as targets for chemotherapy-induced painful peripheral neuropathy. Cytokine. 2012: 59. [CrossRef]
- Cleeland CS, Bennett GJ, Dantzer R, Dougherty PM, Dunn AJ, Meyers CA, et al. Are the symptoms of cancer and cancer treatment due to a shared biologic mechanism? A cytokine-immunologic model of cancer symptoms. Cancer. 2003; 97: 2919-2925. [CrossRef]
- Chirumbolo S, Signorini A, Bianchi I, Lippi G, Bellavite P. Effects of homeopathic preparations of organic acids and of minerals on the oxidative metabolism of human neutrophils. A controlled trial. Br Homeopath J. 1993; 82: 227-244. [CrossRef]
