

Craniopharyngiomas: An Appropriate Surgical Treatment based on Topographical and Pathological Concepts
Ruth Prieto 1, †, *![]() , José M Pascual 2, †
, José M Pascual 2, †![]()
- Department of Neurosurgery, Puerta de Hierro University Hospital, C/ Manuel de Falla 1, 28222, Madrid, Spain
- Department of Neurosurgery, La Princesa University Hospital, C/Diego de Leon 62, 28005, Madrid, Spain
† These authors contributed equally to this work.
* Correspondence: Ruth Prieto ![]()
Received: September 11, 2018 | Accepted: September 28, 2018 | Published:October 16, 2018
OBM Neurobiology 2018, Volume 2, Issue 4, doi:10.21926/obm.neurobiol.1804012
Academic Editor: Antonio Meola
Special Issue: Tumors of the Central Nervous System
Recommended citation: Prieto R, Pascual JM. Craniopharyngiomas: An Appropriate Surgical Treatment based on Topographical and Pathological Concepts. OBM Neurobiology 2018; 2(4): 012; doi:10.21926/obm.neurobiol.1804012.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
The optimal treatment of craniopharyngiomas (CPs) represents a neurosurgical challenge, the major reason being their close relationship with the hypothalamus and the third ventricle (3V) boundaries. Nevertheless, CPs are generally defined as “suprasellar” lesions, an inexplicit and frequently defective term. Despite being heterogeneous lesions, CPs are actually characterized by repeating pathological patterns which depend on their point of origin along the pituitary-hypothalamic axis. Surgical plan in tailoring the best treatment strategy needs to take in consideration some critical aspects, including the understanding of the accurate CP-hypothalamus relation. Without firm consensus and proposed guidelines for the appropriated management of CPs, radical removal and conservative resection remain the two opposing therapeutic strategies. However, an increasing leading of opinions stress out these two strategies should be replaced by a tailored plan to pursue the maximal tumor resection while minimizing the likelihood of hypothalamic injury in each case. Based on the accurate definition of the CP-third ventricle floor relationship, our topographical scheme has been proven useful to predict the degree of hypothalamic distortion and adherence to the tumor. This is an essential information to predict the surgical risk associated with radical tumor removal. Apart from the sellar-suprasellar category of CPs which is formed by tumors growing below a non-distorted third ventricle floor (TVF), four major CP topographies can be considered: i) suprasellar-pseudointraventricular CPs, that grow below an intact but upward displaced TVF; ii) suprasellar-secondary intraventricular CPs, which originate below the TVF but break through it and invade the 3V; iii) not-strictly intraventricular or infundibulo-tuberal CPs, which originate within the TVF itself and predominantly expand into the 3V; and iv) strictly intraventricular CPs that wholly develop within the 3V, above an intact TVF. The most extensive and strongest CP-hypothalamic adhesions occur in the secondary intraventricular and infundibulo-tuberal categories. A hypothalamic position around the middle portion of the tumor, an amputated pituitary stalk and an elliptical tumor shape on preoperative MRI are reliable signs to predict a high-risk CP adherence severity level. In the cases with these radiological signs a limited tumor removal is strongly advocated.
Graphical abstract
Keywords
Craniopharyngioma; topography; hypothalamus; third ventricle; adherence; adhesion; infundibulo-tuberal; treatment; trans-lamina terminalis approach; endoscopic transsphenoidal approach
1. Introduction
Defined by the World Health Organization as “benign, partly cystic epithelial tumours”, craniopharyngiomas (CPs) are widely regarded as rare and challenging intracranial tumours, despite their histological classification. Such a major neurosurgical challenge is due to their intimate relation with the hypothalamus and third ventricle (3V) boundaries. Nevertheless, analysis of the underlying CP pathological and topographical features related to this type of tumors is scarce in medical literature. On the one hand, most studies assume the inaccurate concept of a primary suprasellar position for most CPs, even though this heterogeneous type of lesion may develop at any point along the pituitary-hypothalamus axis, from the sella turcica to the 3V. Moreover, it should be kept in mind that almost half of CPs develop at the level of the third ventricle floor (TVF), within the infundibulum and/or the tuber cinereum, regions including the vital hypothalamic nuclei [1,2,3,4,5]. On the other hand, the extreme heterogeneous CP morphology has definitely contributed to thwart a clear identification of the topographical and pathological CP features which allow the definition of those subgroups of cases associating a high surgical risk. The thorough assessment of 3,705 documents relating to CPs, including books, individual well-reported cases, surgical case series and historical case series such as Cushing’s series recorded in the Brain Tumor Registry (n=124) or the pathological series housed in the Narrenturm, Vienna (n=25), has allowed us to study over 5,000 CPs, including brain specimens from non-operated tumors and surgically treated lesions. We have been able to affirm that CPs, despite representing a morphologically heterogeneous type of tumor, are characterized by repeating topographical and pathological patterns that can be differentiated in anatomical studies [4,6,7]. As hypothalamic dysfunction is the major cause of death and serious morbidity following CP surgery, an accurate preoperative definition of the specific anatomical CP-hypothalamus relationship is essential to plan the most appropriate surgical approach and degree of excision for each case. Regarding this issue, we have recently showed that conventional preoperative MRI studies can reliably predict the accurate CP topography and CP-hypothalamus adhesion pattern to be found in the surgical procedure [8,9]. The aim of this review is to present a critical overview of gathered knowledge on topographical and pathological concepts regarding to CPs that should be considered when planning surgical treatment of these complex lesions.
2. Craniopharyngiomas: A Heterogeneous Group of Epithelial Lesions Developed along the Hypothalamic-Pituitary Axis
2.1 Pathological Definition of Craniopharyngiomas: Historical Background
The morphological and pathological heterogeneity of CPs has notably contributed to the difficulty in classifying these lesions throughout history. In the Nineteenth Century, a vast list of ambiguous terms such as medullary sarcoma, carcinoma of the pituitary gland, ependymal papilloma, cystosarcoma, cholesteatoma, and teratoma, were used to refer to lesions growing in the vicinity of the suprasellar area and showing gross pathological features typical of what we currently known as CPs [10,11,12]. This extremely varied terminology has generated a lot of confusion. The first comprehensive classification of tumors related to the pituitary gland was presented in 1893 by Sir Rupert William Boyce (1863-1911), an assistant professor of Pathology at University College of London [13]. Based on the systematic study of 3,000 brain autopsies, he was able to differentiate the category of “pituitary strumas” or glandular neoplasms, from the remaining hypophyseal or infundibular tumors, such as granulomas, teratomas and carcinomas. Boyce used the term “pituitary cyst” for lesions resembling CPs owing to his erroneous assumption that these tumors developed from an excess of pituitary secretion [13].
The pathological entity of CPs was first systematically defined a decade later, in 1904, by the Austrian pathologist Jakob Erdheim (1874-1937) [14]. The confluence of several fortunate circumstances contributed to Erdheim’s definition of CPs as a separate tumor entity. Carl Benda had recently introduced new staining methods for pituitary gland cells that allowed the differentiation of pituitary “strumas” (adenomas) [15]. In addition, Erdheim had shown a particular interest in the pathological alterations involving the pituitary gland since the beginning of his career and was able to study in detail the collection of old brain specimens with pituitary tumors gathered at the Pathological Anatomical Museum in Vienna, nowadays stored at the Narrenturm (the former hospital for insane patients in Vienna) [16,17]. The methodical study of a set of cystic lesions developed at the infundibulum in these brain specimens eventually led him to define the new pathological category of “hypophysengangsgeschwülste” (hypophyseal duct tumor), a term under which he grouped the heterogeneous epithelial growths developing either from the pituitary stalk or from the infundibulum (presumably from the pars tuberalis, the thin layer of glandular adenohypophyseal tissue wrapping around the pituitary stalk and infundibulum) [14,16]. Erdheim showed great originality in relating the presence of squamous epithelial cell nests within the pars tuberalis, with the embryological development of CPs [14]. With brilliant insight, he proposed that these tumors could originate from epithelial cell remnants of Rathke’s pouch (the embryonic primordium of the pituitary gland) or, more accurately, from non-involuted remnants of the craniopharyngeal duct (Rathke’s pouch’s path of migration connecting the embryo’s mouth and TVF at the earliest stages of pituitary gland development) which become included within the pars tuberalis [14,16]. Although CP pathogenesis is still controversial, recent molecular studies support Erdheim’s embryological theory that CPs originate from displaced embryonic stem cells of the primitive stomodeum located along the pituitary-hypothalamic axis [17,18]. In his monumental masterpiece, Erdheim not only defined the CP entity but also characterized the two major histological variants with distinct morphological and molecular features currently considered in the WHO classification: the adamantinomatous (ACP) and the squamous-papillary (PCP) types, for which he suggested a common embryonic pathogenesis [20,21]: The adamantinomatous type consisted of lesions similar to adamantinomas or odontogenic jaw tumors, characterized by strands of a multistratified squamous epithelium with peripheral palisading of nuclei that enclosed sheets of “stellate reticulum” and cysts filled with cell debris and cholesterol particles. The squamous-papillary type included lesions similar to papillomas of the oral mucosa, typically formed of a unilocular cyst, whose inner wall was lined with a squamous epithelium forming wart-like or cauliflower-like excrescences [16]. Finally, Erdheim also pionnered the relationship between the damage of the infundibulo-tuberal area by CPs and the presence of obesity observed in many patients [22,23,24].
Three decades later, in 1929, the founding father of scientific neurosurgery, Harvey Cushing (1869-1939), introduced the easy-to-remember term “craniopharyngioma” [25]. Despite these lesions not originating from the pharynx but rather from embryo’s primitive buccal cells migrating with Rathke’s pouch/craniopharyngeal duct, the term “craniopharyngioma” eventually triumphed over Erdheim’s more accurate term of “hypophyseal duct tumors” [12,25]. The heterogeneity of CPs regarding their location and their varied extent of adhesion to the surrounding brain structures, commonly led to either failed craniotomies and/or to a high rate of death or life-ruining hypothalamic symptoms, that puzzled Cushing throughout his career. For this reason, he defined CPs as the “most baffling problem which confronts the neurosurgeon” [26]. One century later, CPs remain one of the most formidable and challenging intracranial tumors faced by practitioners.
2.2 Craniopharyngioma: Not a Suprasellar but a True Hypothalamic Tumor
CPs have been classically claimed to represent a suprasellar, extra-axial type of epithelial lesion. Unfortunately, the term “suprasellar” remains invariably linked to the concept of CPs, and it still dominates the neurosurgical and neuroradiological literature on these tumors [20,27,28]. The widespread use of the term “suprasellar” for CPs dates back to the early 20th Century, when the identification of dense shadows above the sella turcica represented the major radiological sign to ascertain the preoperative diagnosis of these lesions [25,26]. The problem posed by this imprecise term is that it may lead to inaccurate topographical definition of the tumor, and consequently to an incorrect surgical decision, as it misses the fundamental point: “the tumor involvement of the vital hypothalamus”. The systematic study of anatomical CP relationships in both surgical and pathological cases published in the literature has proved that this tumor type predominantly involves the 3V and encroaches upon the hypothalamus [3,6,7].
Percival S. Bailey (1892-1973), one of Cushing’s most talented assistants, had a particular interest in neuropathology and was the first author to define CPs as true hypothalamic tumors [29]. The methodical study of Cushing’s vast collection of CP specimens, in addition to Bailey’s interest in hypothalamus physiology, led the latter to notice that most CPs developed within the hypothalamic region and predominantly extended into the 3V [10,29]. Bailey also recognized that diabetes insipidus, adiposogenital dystrophy (Fröhlich’s syndrome) and hypersomnia were all typical symptoms in CP patients that revealed hypothalamic involvement by the tumor [29]. Comprehension of the close relation between CPs and the hypothalamus was crucial for further developing surgical strategies aimed at minimizing the likelihood of devastating hypothalamic injury associated with CP surgery. In 1938, Norman M. Dott (1897-1973), another Cushing fellow who worked with Bailey in Boston, reported the first account of the successful surgical treatment of CPs centered at the hypothalamus [30,31]. Dott proposed a novel strategy, including a two-stage approach (a subfrontal route followed by a transcortical-transventricular approach) to remove both the suprasellar and the intraventricular components of the tumor under direct view. He also warned about leaving untouched the basal portion of the tumor strongly adhered to the TVF in order to avoid undue injury to the adjacent hypothalamus [30].
The following generation of British neurosurgeons, headed by Douglas Northfield (1902-1976), contributed to emphasize the concept of a true hypothalamic, tuberal topography for a large number of CPs. Based on the ischemic/hemorrhagic lesions found within the hypothalamus in the autopsy of patients who died following surgical attempts at removal of CPs originated in the infundibulo-tuberal region, Northfield warned about the impossibility of resecting those lesions growing in the basal hypothalamus [32]. Recent studies focusing on the meningeal relationships between CPs and the pituitary-hypothalamic axis in a large series of tumors reported by Song Tao Qi et al. found that a subarachnoid-subpial position of the lesion within the TVF, without any intervening membranous layers between the tumor and the hypothalamus, occurred in 30% and 50% of pediatric and adult patients, respectively [5,33,34]. In light of the aforementioned information, the generalized and misleading term “suprasellar” should be abandoned and substituted by an accurate description of CP topography.
3. Topographical Classifications of Craniopharyngiomas
Numerous classification schemes for CP topography have been proposed. Table 1 summarizes the major twenty-six topographical schemes published in the literature since this entity was defined in 1904 to the present. These series include a total of 2,480 CP cases. In most of them, surgical evidence represented the principal source of information [35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58]. Only six classifications were based on the pathological evidence of the relationships between the tumor and adjacent intracranial structures identified on brain autopsy specimens [1,4,5,6,14,32,33,34,59,60,61,62]. Among these schemes, the one presented by Juraj Steno in 1985 deserves special attention because it is the first modern topographical classification based on the anatomopathological features of 30 brain specimens of non-operated CPs [1]. Stenos’ scheme takes into consideration the degree of TVF involvement by the lesion, classifying CP topography into three major types: i) purely extraventricular lesions developed in the sellar and/or suprasellar compartments outside the 3V; ii) extraventricular-intraventricular CPs that grow in both the suprasellar cistern and the 3V cavity, in which the TVF remnants are located around the mid-third of the tumor; and iii) purely intraventricular CPs wholly developed within the 3V above an intact TVF [1]. Shortly afterwards, Ivan S. Ciric published the only CP classification based on the embryological development of the leptomeningeal layers and their relative position with the epithelial remnants of Rathke pouch cells [63]. Ciric’s scheme included a depth axis from the outer meningeal layers to the inner nervous tissue and distinguished three groups of lesions: i) extrapial-intrarachnoid CPs, separated from the TVF tissue by the arachnoid and pia layers; ii) partially intrapial CPs, growing inside the nervous tissue of the TVF; and, iii) completely intrapial CPs, developing purely inside the 3V above an intact TVF. Finally, several topographical schemes are mainly based on MRI studies, including the two French classifications discussed below [64,65,66,67].
In the early 1990s, the neuroradiologist Charles Raybaud differentiated four major anatomic regions that could be occupied by the tumor: the sellar; suprasellar; infundibulo-tuberal; and third ventricle compartments. He observed that the majority of CPs primarily develop in the infundibulo-tuberal region, and his classification was the first MRI-scheme supporting the concept that CPs represent a type of lesion primarily involving hypothalamus [64], as had been previously found in the autopsy studies led by Erdheim and Steno [1,14]. More recently, Christian Sainte-Rose and Stephanie Puget introduced a topographical CP scheme based on the appearance of the hypothalamus on preoperative MRI scans, which also took into consideration patient outcome [66,67]. This scheme distinguished three major degrees of hypothalamic distortion caused by the tumor: i) grade 0, which corresponds to cases without hypothalamus distortion; ii) grade 1, included tumors causing hypothalamus displacement; and iii) grade 2, formed by tumors encroaching upon the hypothalamus, which cannot be identified on preoperative MRI [66,67]. Saint-Rose and Puget’s scheme, however, has the drawback of assuming that the 3V involvement depends on the progressive expansion of a tumor theoretically originated at the sellar/suprasellar region, without taking into consideration the multiplicity of CP locations along the pituitary-hypothalamic axis. Furthermore, the appearance of the TVF on preoperative MRIs cannot be used as a valid sign to reliably ascertain the anatomical integrity of this structure. For example, an unidentifiable TVF does not necessarily signify its anatomical disruption by the tumor. In a recent study analyzing the anatomical CP relationships for a series of 17 intraventricular CPs, it was found that 15% of the cases whose TVF could not be identified on preoperative MRIs actually corresponded to purely intraventricular CPs presenting a small pedicle attachment to the intact TVF, a low-risk adhesion type allowing a safe radical removal [5].
3.1 Topographical Craniopharyngioma Schemes: Anatomical Reference Axes Used
According to the anatomical axis considered for CP classification, four major types of topographical CP schemes can be distinguished (Table 1):
Topographical classifications considering one vertical axis. A total of 12 series considered the occupation of the compartments along the vertical sellar-3V axis (sellar, suprasellar, infundibulo-tuberal and 3V) as the main criterion for CP classification [14,32,41,42,43,45,46,47,48,49,50,51,52,53,54,57,59,64,65,66,67]. The problem with many of these schemes is that they may lead to the erroneous idea that all CPs originate within the sella/suprasellar area and then progressively expand towards the 3V as they enlarge. Rather, different potential primary sites of CP development should be contemplated.
Table 1 Summary of the major topographical classifications of craniopharyngiomas

Topographical classifications considering one horizontal or antero-posterior axis. Two classic surgically-based schemes used the optic chiasm to classify the position of CPs, as this was the main anatomical structure indefied through the frontotemporal or pterional approach [35,36,39,40]. These schemes distinguished three major CP topographies: i) prechiasmatic CPs―for tumors originated below the chiasm which expand between both optic nerves; ii) subchiasmatic CPs―for the tumors displacing the optic nerves and chiasm upwards; and iii) retrochiasmatic CPs―for lesions hidden behind the optic chiasm and pushing this structure forward, most of them expanding within the 3V. The problem with the term “retrochiasmatic” is that it does not provide any information about the accurate relationship between the tumor and the 3V-hypothalamus in these schemes.
Topographical classifications considering two axes: one vertical or lateral and one horizontal. Five CP classifications are based on the vertical and antero-posterior axes [37,38,44,55,56,60,61], and two schemes consider the lateral position of the tumor relative to the pituitary stalk in addition to either an antero-posterior axis [68,69] or a vertical axis [58]. For example, William H. Sweet (1910-2001), who advocated the pterional-trans-lamina terminalis route for CPs, proposed a scheme based on the tumor position relative to the optic chiasm and 3V. Very recently, Amin K. Kassam [55] and Bin Tang [58], two experts in the endoscopic extended transsphenoidal approach, used the pituitary stalk and infundibulum as the structures of reference to define CP topography, due to the fact that they are the first ones identified when using the transsphenoidal route. Specifically, Kassam’s scheme considers four major CP types [55]: i) preinfundibular CPs, or lesions located in front of the stalk-infundibulum complex, just behind the optic chiasm; ii) transinfundibular CPs, tumors expanding into the pituitary stalk itself; iii) retroinfundibular CPs, corresponding to those lesions growing behind the stalk-infundibulum complex which can expand either into the 3V cavity or towards the suprasellar-interpeduncular compartments; and iv) intraventricular CPs, situated above an intact pituitary stalk. The removal of this last type through an endonasal transsphenoidal route necessarily compels breaking through an anatomically intact TVF.
Topographical classifications considering two axes: one vertical and one depth axis through the leptomeningeal-brain tissue complex forming the TVF. Four studies classified the tumor location along the vertical pituitary-hypothalamic axis in addition to considering how deeply the tumor extended into the leptomeningeal layers and nervous tissue [1,3,4,5,6,33,34,62,63,70,71]. Steno’s scheme was the first to highlight that the presence of an intervening meningeal layer between the tumor and the outer-pial aspect of the TVF in CPs developed beneath an intact TVF allowed a straightforward and safe removal of these tumors, except in recurrent cases [1,2]. A safe radical removal could be also achieved in purely intraventricular CPs in which the TVF was found to be anatomically intact below the lesions. On the contrary, he noticed that the highly prevalent group of CPs with an extra-intraventricular position, formed by lesions centered at the TVF, was characterized by direct contact between the tumor and the hypothalamus. The strong adhesions between these tumors and the surrounding TVF explain the highest surgical risk of hypothalamic injury when attempting a radical removal of this CP topography [1]. The recent surgical classifications proposed by Pascual et al. and Qi et al. [4,5,6,33,34,62] integrate the pathological concepts evidenced in Steno’s seminal study [1] with the embryological theory proposed by Ciric [63]: that those CPs developing within the neural tissue of the infundibulum/tuber cinereum are originated from Rathke’s pouch cell remnants coming into contact with the diencephalic vesicle floor before the pia mater is wholly developed and covers the basal brain surface.
3.2 Topographical Craniopharyngioma Classification Based on the Assessment of the Third Ventricle Floor Status: Surgical Implications of Our Model
The most important aspect when planning CP surgery is to well understand the anatomical position of the hypothalamus relative to the tumor, with the aim of predicting the likelihood of achieving a safe resection. In this regard, in 2004, our group presented a comprehensive classification scheme for CPs based on the definition of the accurate anatomical relationships between the tumor and the TVF, the region containing hypothalamic nuclei. This anatomical area is essential for monitoring vital functions such as food intake, body water homeostasis, primary emotional reactions of aversion/craving, as well as the control of the sleep-wakefulness cycle [6]. Four major CP topographies depending on the specific type of CP-TVF relationship were identified: i) suprasellar-pseudointraventricular CPs: the category of lesions usually originated at the junction between the pituitary gland and stalk that expand within the suprasellar cistern while causing an upward displacement of the TVF, mimicking an intraventricular position; ii) sellar/suprasellar-secondary intraventricular CPs: lesions initially develop under the 3V but at later stages invade and occupy the 3V cavity after breaking through the TVF; iii) infundibulo-tuberal or not-strictly intraventricular CPs: tumors developed at a subpial position within the neural layer of the infundibulum or tuber cinereum and expanding predominantly into the 3V (these lesions grow in close contact to the hypothalamic nuclei [3,4]); and iv) strictly-intraventricular CPs: tumors primarily developed within the 3V, above an intact TVF [4,6,62]. An additional topographical category of CPs without 3V involvement has to be considered, the group of sellar-suprasellar CPs that includes those tumors originated at the dorsal surface of the pituitary gland, beneath the sellar diaphragm, which exclusively occupy the sellar and/or suprasellar compartments (Figure 1). This scheme is relatively simple and has the major advantage of providing essential information about the type of hypothalamic-CP relationship that will be found during the surgical procedure. Furthermore, the relative position of the hypothalamus and its degree of anatomical distortion can be easily ascertained on preoperative MRI studies by defining the CP topography according to these categories [8,9]. In our topographical scheme, the category of sellar-suprasellar CPs is the one associating the lowest risk of hypothalamic injury, whereas the surgical risk is maximal for the secondarily-intraventricular and infundibulo-tuberal topographies that are characterized by wide and strong adhesions to the hypothalamus [7].
Figure 1 Topographical classification scheme for craniopharyngiomas based on the original point of development along the hypothalamic-hypophyseal axis [3,6]. Left: Illustrative mid-sagittal schematic of the hypothalamic-hypophyseal complex. The lower part of the hypothalamus surrounding the infundibular recess (IR) corresponds to the infundibulum. CPs may originate at four different points along this vertical axis: i) at the dorsal surface of the pituitary gland (1); ii) from the pars tuberalis covering the infundibular stem or pituitary stalk (2); iii) at a subpial position within the neural tissue of the median eminence (ME) and the tuber cinereum (TC) of the third ventricle floor (3); iv) wholly within the third ventricle, from beneath the ependymal layer of the infundibulum (4). A: arquate nucleus; Ch: optic chiasm; DM: dorsomedial nucleus; ds: diaphragma sellae (in blue); M: medial mammillary nucleus; MB: mammillary body; P: posterior nucleus; PD: pars distalis; PI: pars intermediate; PN: pars nervosa; PV: paraventricular nucleus; SO: supraoptic nucleus; TM: tuberomammillary nucleus; VM: ventromedial nucleus; 3V: third ventricle. Right: Tumor-hypothalamus anatomical relationships for the five major CP categories considered in our topographical classification: i) sellar-suprasellar; ii) sellar/suprasellar pseudointraventricular (S-SS-Pseudo 3V); iii) sellar/suprasellar secondary intraventricular (S-SS-Secondary 3V); iv) not-strictly intraventricular (Not-strictly 3V) or infundibulo-tuberal; v) strictly intraventricular (strictly 3V). Column A shows the tumor-hypothalamus relationships as observed on mid-sagittal MRI scans. Column B illustrates these relationships as seen in coronal trans-infundibular sections. The position of the hypothalamus (in red) relative to the tumor is indicated for each topographical category. The color of the frame for each topographical category corresponds to the number of the point of origin along the hypothalamic-hypophyseal axis.
3.3 The Category of Infundibulo-tuberal Craniopharyngiomas: Clinical Assessment and Surgical Risks
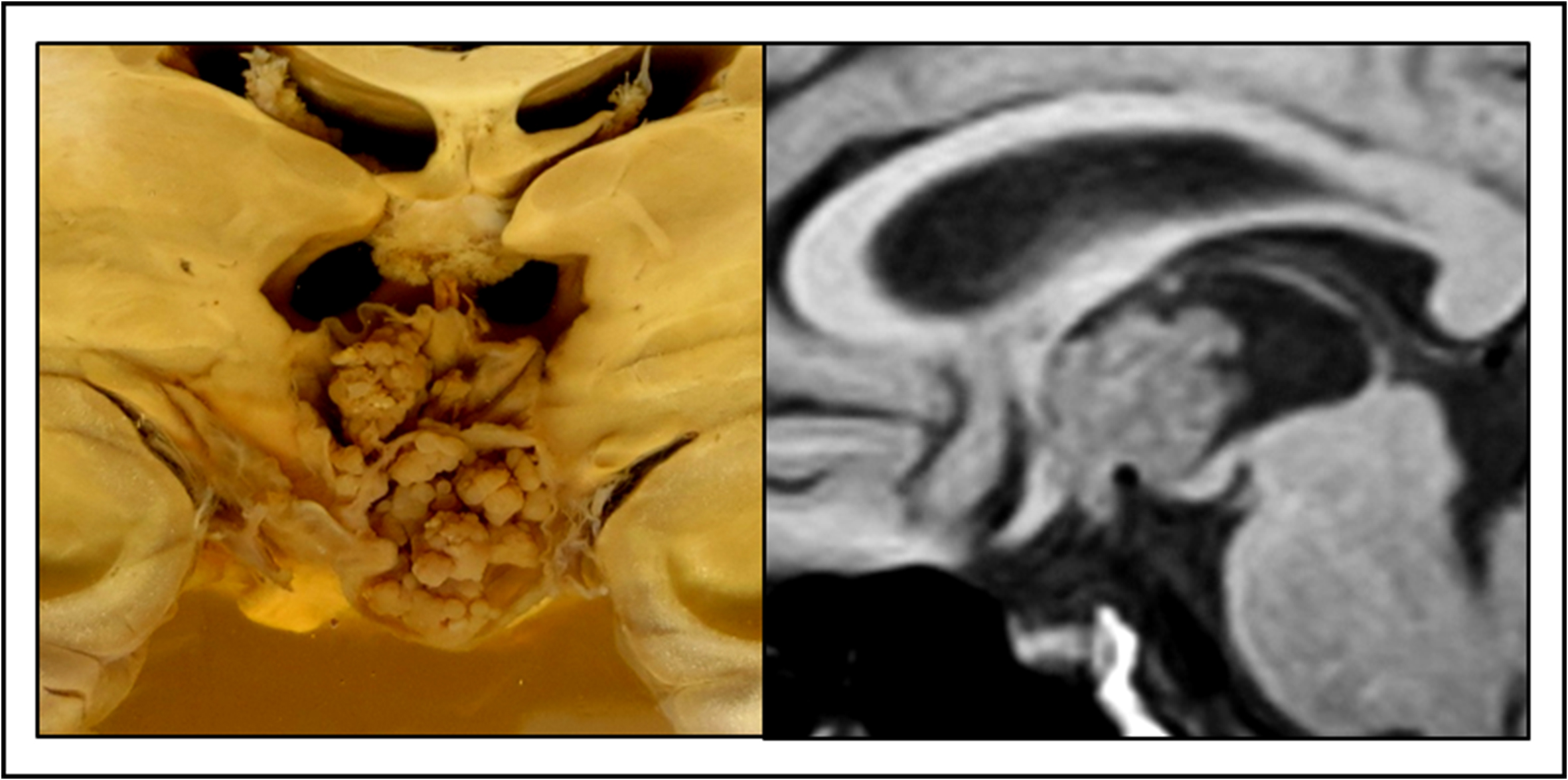
The category of not-strictly intraventricular or infundibulo-tuberal CPs deserves special address due to the fact that it is the most prevalent topography in both adults and children, with an overall rate between 30 and 50% of cases, and the one associating the highest surgical risk [1,6,33,42,52,53,54,72]. Infundibulo-tuberal CPs originate in the basal region of the hypothalamus within the TVF, an anatomical area formed by the infundibulum (Figure 1), the hollow and funnel-shaped proximal portion of the neurohypophysis, and the tuber cinereum, the adjacent grey matter enclosed between the optic tracts and the mamillary bodies [30,75]. Mortality rates reported for this topography range between 4 and 15%, and postoperative morbidity due to hypothalamic injury, including lethargy, apathy, progressive obesity, severe memory loss, and behavioral or psychiatric disturbances may occur in up to 50% of patients, whose quality of life becomes notably hampered [76]. The underlying reason for such a high risk of hypothalamic damage is the subpial origin of this CP category leading to the close contact between the tumor capsule and the hypothalamic nuclei, without any protective intervening meningeal layer.
The median eminence (Figure 1), located along the midline of the infundibulum, contains the arcuate nucleus, which plays a fundamental role in the regulation of feeding behavior linked to energy balance. In addition, the lower ventromedial, periventricular and tubero-mamillary nuclei, as well as the supra-optic-hypophyseal and tubero-hypophysial tracts included within the infundibulo-tuberal region are involved in the regulation of water metabolism, control of sleep cycles and sexual functions through the monitoring of circulating sexual hormones and the control of hypophyseal secretion of gonadotropins [30,77,78,79,80,81]. Apart from a thorough assessment of MRI studies, the preoperative identification of symptoms caused by dysfunction of these hypothalamic basal structures is essential to predict the anatomical and functional status of the infundibulum and tuber cinereum. The infundibulo-tuberal syndrome can be observed in patients with a functional impairment of the infundibulum and tuber cinereum, and is manifested by symptoms such as abnormal somnolence, diabetes insipidus and/or adipose-genital syndrome [82]. This adipose-genital syndrome, also known as Fröhlich’s syndrome, consists of sexual infantilism and abnormal obesity [23]. Despite the surgeon’s experience and clinical skills, any forcible attempts at radical CP removal in patients with symptoms of the infundibulo-tuberal syndrome can lead to a high risk of irreversible hypothalamic injury and severe postoperative morbidity or even patient death [4,65,82].
The infundibulo-tuberal CP topography makes the greatest controversy regarding the feasibility of achieving a radical resection. Some surgeons, led by William H. Sweet (1910-2001) considered the layer of gliosis developed around these tumors as a viable cleavage plane for a safe and radical removal [44,84]. On the contrary, histological/pathological evidence has shown a true fusion between the tumor and the surrounding hypothalamus, rendering a total excision impracticable. The generation of a sticky layer of reactive gliosis at the TVF remnants around the tumor additionally contributes to the strong, extensive adhesions usually found in this subgroup [83]. Both Bailey and Northfield emphasized that extreme adhesiveness of the glial layer was a sign indicating that the cleavage plane was positioned within the normal hypothalamus [29,59]. Actually, the overall rate of total resection for the infundibulo-tuberal category is only about 60%, a percentage notably lower than that reported for other CP categories. This indicates the difficulty of releasing the tumor from the hypothalamic adhesions and/or the neurosurgeon’s determination to leave untouched the tumor fragments strongly attached to the floor/walls of the 3V in these cases [76]. In support of such a conscious decision, Kubota’s et al. analysis of the brain-tumor interphase in 6 whole CP specimens predominantly growing inside the 3V found that the layer of peritumoral gliosis had an irregular thickness and, in some areas, no effective distance for a safe dissection could be identified between the tumor and the adjacent hypothalamic nuclei [73]. Likewise, several authors have evidenced the presence of tumor finger-like protrusions penetrating into the adjacent hypothalamus [85,86,87], a decisive histological finding suggesting the cautious assessment of CP-hypothalamus adhesions and warning against the indiscriminate radical removal of infundibulo-tuberal CPs.
4. Craniopharyngioma Adherence: From a Neurosurgeon’s Subjective Notion to an Objective Definition of Adhesion Pattern and Severity
Apart from the neurosurgeon’s skill, patient outcome following CP removal mainly depends on the type and strength of tumor adhesion to the hypothalamus [7,88]. The pervasive uncertainty regarding the extent and degree of adhesion in each case is a source of great distress for the neurosurgeon. The extreme heterogeneity of tumor adhesions has surely contributed to the lack of a reliable description of this pathological feature in most modern CP surgical series. We have recently been able to address this issue through the methodical examination of 500 well-described CPs, including non-operated whole tumors from brain autopsy specimens as well as surgically treated cases. We were able to identify repetitive patterns of CP adhesion associated with specific tumor topographies and to present the first comprehensive classification of CP adherence [7]. Furthermore, our methodology allows for an accurate, reliable assessment of the pattern and strength of CP adhesions employing conventional MRI studies [9]. This model provides an objective way of grading the type of CP-hypothalamus adhesions into five major levels of severity, each one associating an increasing risk of hypothalamic injury during surgery. A critical understanding of surgical risks based on the severity of CP adhesions to the hypothalamus defined on preoperative MRI may be a fundamental tool for guiding the neurosurgeons’ decision regarding the safest approach to the tumor and extent of removal to be carried out in each patient [7,9].
4.1 The Three Components of Craniopharyngioma Adherence
The type of tumor adherence can be objectively defined according to three components:
Anatomical structures involved in the adhesion. This component defines the structure of the hypothalamic-pituitary axis to which the tumor shows the predominant or primary adhesion. The maximal adhesion is usually observed at the anatomical structure where the CP originally develops. According to the anatomical structure involved, the following types of attachment can be differentiated (Figure 2): i) attachment to the pituitary gland and/or sella turcica, below the diaphragm sellae; ii) attachment to the pituitary stalk and outer surface of the infundibulum; iii) attachment to the entire thickness of the TVF; iv) attachment to the TVF and 3V walls; v) attachment to the ependymal lining of the 3V; vi) attachment to the whole hypophyseal-hypothalamic axis.
Morphological pattern of CP adhesion. This component defines the extent and shape of the CP adhesions, and six patterns can be distinguished (Figure 3): i) pedicle-like attachment, formed by a narrow fibro-vascular stem between the tumor base and the ependyma of the 3V, usually observed in purely or strictly intraventricular CPs; ii) sessile or “patch-like” attachment, in which a limited area of the tumor surface forms the adhesion, usually to the pituitary stalk and/or infundibulum; iii) “cap-like” adhesion, involving the upper half of the tumor, usually visible in large CPs pushing the 3V upwards (pseudointraventricular CPs); iv) ring-like attachment, in which a band of adhesion encircles the tumor’s central portion, usually observed in tumors invading the 3V (secondarily 3V CPs) and also in CPs developed within the TVF itself (infundibulo-tuberal CPs). As this band of adhesion is usually formed by the nervous tissue remnants of the TVF, it represents a close, hazardous-to-touch plane contact between the CP and the hypothalamus; v) “bowl-like” adhesion, in which the tumor’s bottom part is attached to the TVF, observed among CPs expanding within the 3V; vi) circumferential adhesion, the most extensive type of attachment in which the surrounding brain tissue wraps around the entire tumor surface, typical of infundibulo-tuberal CPs.
Figure 2 First component of craniopharyngioma adherence: intracranial structures involved in the attachment [7]. Six major adhesion patterns can be considered: A. Sella-Gland: tumor attachment occurs within the sella turcica to the pituitary gland and/or the sellar structures below the diaphragm sellae. B. Outer aspect of the Stalk-Infundibulum: the CP attachment occurs at the solid portion of the pituitary stalk and the outer aspect of the infundibulum. C. Third ventricle floor (TVF): the tumor is adhered to the entire thickness of the TVF. D. TVF-3V walls: CP attachment involves the floor and walls of the third ventricle. E. 3V (inner lining): the tumor is attached to the ependymal lining of the third ventricle cavity. F. Global (Sella to 3V): the CP attachment involves all the structures of the hypophyseal-hypothalamic axis.
Figure 3 Second component of craniopharyngioma adherence: morphology or extent of the attachment [7]. Six major patterns can be distinguished: A. Pedicle: the tumor is attached through a narrow fibrovascular stem. B. Sessile: small patch of adhesion. C. Cap-like: wide adhesion involving the upper half of the tumor. D. Ring-like: a circular band of brain tissue (the TVF) is encircling the central portion of the tumor surface. E. Bowl-like: wide adhesion to the infundibulo-tuberal region involving the lower half of the tumor. F. Circumferential: the entire tumor surface is attached to the surrounding brain tissue (hypothalamus).
Strength of CP adhesion. This component describes the resistance offered by the attachment to surgical release and can be classified in four types (Figure 4): i) loose or easily dissectible adhesions; ii) tight adhesions, for which a sharp dissection is required to preserve the anatomical structure attached; iii) CP-brain or CP-pituitary stalk fusion, when there is no identifiable cleavage plane between the tumor and the adjacent nervous tissue; iv) replacement, the strongest and most dangerous degree of adhesion occurs when the structure involved in the attachment is no longer recognizable because it has been replaced by tumor growth. The infundibulum and tuber cinereum of the TVF are usually replaced by large infundibulo-tuberal CPs as well as by secondarily 3V lesions encroaching upon the 3V.
Figure 4 Third component of Craniopharyngioma adherence: adhesion strength [7]. Four major patterns can be identified: A. Loose: easily dissectible adhesion. Note the arachnoid layer (arrows) interposed between the tumor (t) and the normal brain; B. Tight: No meningeal layer is interposed between the tumor (t) and the anatomical structure. Sharp tumor dissection is mandatory to preserve the brain structure attached. PG: pituitary gland; PS: pituitary stalk; C. Fusion: a cleavage plane between the tumor and the adjacent brain tissue cannot be identified; D. Replacement: the structure involved in the attachment is no longer recognizable, as it has been encroached upon and replaced by the tumor. Ch: optic chiasm; MB: mamillary body.
4.2 Craniopharyngioma Adhesions Classified into Five Levels of Adherence Severity
Taking into consideration the three components of tumor adhesion, the severity of CP adherence can be classified into 5 major levels—mild, moderate, serious, severe, and critical (Figure 5)—each associating an increasingly higher risk of hypothalamic injury and a worse postoperative outcome [7]. The least severe type of hypothalamic adhesion (level I or mild) occurs more often in wholly intrasellar or sellar-suprasellar CPs separated from the TVF by a meningeal layer, either the dura mater of the diaphragm sellae or the arachnoid membranes of the chiasmatic cistern. Level II or moderate severity is typically observed in strictly intraventricular CPs with a pedicle or a sessile attachment to the ependymal lining of the 3V, a type of adhesion which can usually be released straightforwardly. Level III (serious) adhesion is found in suprasellar CPs tightly adhered or fused to the pial surface of the infundibulum and/or tuber cinereum, without any intervening arachnoid layer. Attempts at releasing the tumor from these adhesions to the outer surface of the median eminence/basal hypothalamus associated a poor outcome in about one tenth of the cases. Level IV (severe) occurs in CPs fused to the TVF nervous tissue or those replacing the infundibulo-tuberal region. These extensive adhesions to the hypothalamus are usually observed in infundibulo-tuberal CPs and in tumors invading the 3V. Severe CP adhesions usually show a bowl-like, ring-like or circumferential morphology, and forceful attempts to separate the tumor from the adjacent hypothalamus led to a poor outcome in about 25% of cases due to irreversible hypothalamic damage. Finally, level V, the most severe (critical) degree of hypothalamic adherence occurs in large and aggressive CPs extending from the sella to the 3V roof that encroach upon all the structures of the pituitary-hypothalamic axis. The invasion and replacement of the TVF led to a rate of poor outcome/death as high as 40% in this group [7].
Figure 5 Severity levels of craniopharyngioma adherence to the hypothalamus. The first row shows autopsy specimens of CPs (t) for the five adherence severity levels (I to V) considered. The middle and lower rows display preoperative and postoperative MRI scans, respectively, of tumors presenting similar adherence severity levels to those shown in the autopsy specimens. The red arrows point to the position of the hypothalamus relative to the tumor. The table at the bottom summarizes the specific three components of CP adherence that define each level of severity. Level I - Mild: A1. Midsagittal brain section showing a sellar-suprasellar CP (t) which displaced the third ventricle floor upward (red arrow). MB: mamillary body; 3V: third ventricle. A2. Preoperative midsagittal section showing a sellar-suprasellar CP (t). Note the hypothalamus (red arrow) is above the tumor. Ch: optic chiasm. A3. Postoperative scan demonstrating the anatomical integrity of the third ventricle floor (TVF) following radical tumor removal through a pterional route. Level II - Moderate: B1. Coronal autopsy specimen showing a strictly intraventricular papillary CP (t) with a small basal attachment (blue arrow) to the TVF (red arrows). B2. Preoperative MRI scan of a solid strictly intraventricular CP (t). Note the pituitary stalk (PS) and the pituitary gland (PG) are intact below the tumor. B3. Postoperative scan demonstrating an intact TVF following a complete tumor resection through a pterional trans-lamina terminalis approach. Level III - Serious: C1. Sellar-suprasellar pseudointraventricular CP (t) beneath an upwardly displaced TVF (red arrow). C2. Preoperative midsagittal MRI scan showing a pesudointraventricular CP (t) pushing the TVF upward and stretching the chiasm (Ch). C3. Contrast-enhanced areas can be observed at the upper pituitary stalk (PS) and the outer side of the infundibulo-tuberal area (arrows), a sign of residual tumor/gliotic scarring after blunt dissection of a tightly attached tumor which was approached through a pterional route. Level IV - Severe: D1. Not-strictly intraventricular or infundibulotuberal CP (t) with a mixed solid-cystic consistency. Note the MB is the only visible TVF structure. The pituitary stalk (PS) has been amputated by the tumor and the pituitary gland (PG) is intact beneath the tumor. D2. Coronal preoperative MRI scan showing an infundibulo-tuberal CP (t). The hypothalamus is located around the mid-third portion of the tumor (red arrows). D3. Postoperative scan revealing a hypointense sign on the left hypothalamus (arrow), indicating hypothalamic injury after radical trans-lamina terminalis tumor resection. Level V - Critical: E1. Sagittal section showing a suprasellar-secondary intraventricular CP (t) that has broken into the third ventricle. E2. Preoperative MRI scan showing a large multilobulated secondary intraventricular CP (t). The hypothalamus (red arrows) is around the mid-third portion of the tumor. E3. Postoperative contrast-enhanced T1-weighted MRI scan, following a radical transcallosal removal, shows a breached TVF (asterisk), a sign suggesting tumor replacement of the tuber cinereum. The hyperintense sign at the TVF remnants (arrow), indicates the presence of gliotic scarring and/or tumor remnants.
5. Diagnosis of CP Topography: MRI Predictors of the Tumor-Hypothalamus Relationship
Since the introduction of MRI in the late 1980s, this technology represents the gold standard tool for the preoperative diagnosis of CPs, despite CT remaining more useful to depict tumor calcifications. MRI allows an accurate assessment of the tumor’s anatomical relationships in the three spatial dimensions [89]. Preoperatively recognizing the true hypothalamus position regarding the tumor, as well as the anatomical distortion of this structure, represents essential information for the neurosurgeon to anticipate the risks of hypothalamic injury and to plan accordingly the most suitable surgical procedure. Our group has recently demonstrated that an accurate definition of CP topography (Figure 6) and the type of CP-hypothalamus adhesion (Figure 7) can be reliably achieved with conventional MRI by examining the T1- and T2-weighted sequences [8,9]. Midsagittal and coronal-transinfundibular MRI sections are the two most important ones for a proper assessment, as CPs originate along the midline structures that form the pituitary-hypothalamic axis. By assessing a small set of MRI signs, it is possible to achieve a correct preoperative definition of CP topography and hypothalamic adhesion severity in a high rate of patients, 85% and 90% of cases respectively [8,9]. Preoperative MRI evaluation must include the occupation by the tumor of the intracranial anatomical compartments surrounding the pituitary-hypothalamic axis (sella turcica, chiasmatic-or suprasellar- cistern and 3V), in addition to the anatomic distortion of the pituitary-hypothalamic structures (pituitary gland, pituitary stalk, infundibulum, tuber cinereum and 3V walls).
5.1 Tumor Occupation of the Third Ventricle and the Chiasmatic Cistern
The compartments whose occupation provide the most reliable information to define CP-hypothalamus relationships are the 3V and the chiasmatic-or-suprasellar cistern. No occupation of the 3V is only observed in the sellar-suprasellar topography, the one associating the lowest risk of hypothalamic injury (Figure 6. A1). Although extremely important, accurately distinguishing between the four remaining topographical categories involving the 3V is more difficult, and the occupation of the chiasmatic cistern represents one of the most valuable radiological signs. A wholly tumor-free chiasmatic cistern strongly points to the strictly intraventricular topography (Figure 6. E1), whereas its partial occupation (“belly-like” protrusion of the TVF) is typical of the infundibulo-tuberal category (Figure 6 D1). Complete obliteration of the chiasmatic cistern may be observed in tumors originated below the TVF (suprasellar-pseudointraventricular or secondary intraventricular topographies) (Figure 6. A1, B1, C1) [8].
5.2 Pituitary Stalk Distortions
The anatomical distortions of the pituitary-hypothalamic axis, in particular the appearance of the pituitary stalk and the anatomical position the hypothalamus relative to the tumor, are the two most useful MRI signs to define the type of CP-hypothalamus relationship. The appearance of the pituitary stalk is the radiological sign showing the strongest correlation with the type of CP topography [8]. Four major patterns of stalk distortion can be differentiated on preoperative MRI scans: intact or wholly visible; thickened; amputated; and not visible. Amputation of the upper infundibular portion of the stalk by the tumor is usually observed in the not-strictly intraventricular or infundibulo-tuberal topography (Figure 6. D1). This sign strongly suggests the presence of a severe (level IV) CP adhesion to the hypothalamus. On the contrary, a normal pituitary stalk appearance points to the strictly intraventricular topography with a moderate (level II) adherence to the hypothalamus (Figure 6. E1). Inability to identify the pituitary stalk on preoperative MRI is a less specific sign, as this can occur in any of the three CP topographies that originate beneath the TVF and occupy the chiasmatic cistern: the sellar-suprasellar, pseudointraventricular and secondary intraventricular topographies, all of which encroach upon the whole pituitary stalk (Figure 6. A1, B1, C1).
5.3 Hypothalamus Position Relative to the Tumor
The level of the hypothalamus relative to the tumor is the most informative MRI sign to predict the severity of CP adherence [9]. This variable is best assessed on coronal-transinfundibular MRI sections, and three major positions can be considered: hypothalamus located at the bottom of the tumor area; around its mid-third portion; or above the top pole of the lesion. When the hypothalamus is located around the mid-third or central portion of the tumor, the presence of extensive and tenacious adhesions to the hypothalamus, with either a ring-like or a circumferential pattern (high-risk adherence levels, IV-severe or V-critical), should be expected (Figure 7. D2, E2). On the contrary, when the hypothalamus is located either around the lower third (Figure 7. B2) or upper third of the tumor (Figure 7. A2, C2), low-risk adherence levels (I-mild, II-moderate, or III-serious) are likely to be found [9]. A hypothalamus positioned at the lower third of the tumor is typically observed in the strictly intraventricular topography (Figure 6. E2), whereas a hypothalamus situated above the tumor pole generally occurs in the sellar-suprasellar (Figure 6. A2) or pseudointraventricular (Figure 6. B2) topographies [8].
Figure 6 MRI signs defining the five major topographical craniopharyngioma categories. Midsagittal (A1 to E1) and coronal-transinfundibular (A2 to E2) MRI sections representative of each category. Red arrows point to the relative position of the hypothalamus in relation to the tumor. Blue angles formed by the intersection of a plane tangential to the base of the mamillary bodies (MB) with the plane tangential to the fourth ventricle floor forms the mamillary body angle. Ch: chiasm; t: tumor; 3V: third ventricle. The table below summarizes the specific MRI signs observed for each topographical category.
5.4 Craniopharyngioma Shape
Some macroscopic CP features, such as tumor size, consistency, shape, or presence of calcifications, provide key information about the extent and degree of CP adhesions, and should also be defined on preoperative neuroradiological studies. Among these features, tumor shape has proven particularly useful to predict the severity of CP-hypothalamus adhesions. A pear-like tumor outline is typical of CPs originated within the sellar compartment which have pushed the diaphragm sellae upward against the optic chiasm as they grow (Figure 7. A2). The presence of this layer of duramater interposed between the tumor and the TVF prevents the development of tight adhesions to the hypothalamus in these cases, associating the lowest risk of hypothalamic injury. Quite the opposite, a multilobulated morphology indicates that the tumor originated along the PS, at the level of the chiasmatic -suprasellar- cistern, and that it expanded into the arachnoid spaces, giving rise to more extensive and sticky adhesions to the hypothalamus (Figure 7. E2). Finally, the elliptical shape is associated with the tumors showing the most severe degrees of hypothalamic attachment (levels IV and V) (Figure 7. D2) [9]. Two additional, highly informative MRI signs that should be evaluated on preoperative MRI studies are the mamillary body angle and the anatomical distortion of the optic chiasm, both of which will be described below.
Figure 7 Surgical findings and MRI signs defining the five increasing severity levels of craniopharyngioma adherence. The bottom table summarizes the specific MRI signs associated with each CP adherence severity level. Level I - Mild: A1. Right pterional view showing the arachnoid layer (arrow) between the tumor (t) and the surrounding structures. ICA: internal carotid artery; rON: right optic nerve. A2. Midsagittal MRI scan showing a craniopharyngioma with a pear-like morphology (t) expanding in the sellar and suprasellar compartments below the hypothalamus (red arrow). The pituitary stalk cannot be identified. Level II - Moderate: B1. Surgical view through a right pterional approach showing the narrow pedicle attachment (arrow) of a papillary CP (t) to an intact third ventricle floor (TVF) below the tumor. B2. Midsagittal MRI scan of a round solid tumor (t) purely located in the third ventricle. Note the hypothalamus (red arrow) is below the tumor and the pituitary stalk (PS) has a normal appearance. Level III - Serious: C1. Right pterional view showing a tight adhesion (arrow) between the tumor and the upwardly displaced chiasm and third ventricle floor. C2. MRI scan showing a dumbbell CP (t) that displaces the chiasm and third ventricle floor (red arrow) upward, mimicking an intraventricular position. Level IV - Severe: D1. Intraoperative view through a right pterional approach showing a CP (t) fused (arrows) to the inner surface of the infundibulum (IF). D2. Coronal MRI scan showing an elliptical tumor (t) that predominantly expands into the third ventricle and partially occupies the chiasmatic cistern. Note the pituitary stalk (PS) has been amputated. The hypothalamus is positioned around the mid-third of the tumor. Level V - Critical: E1. Intraoperative view through the lamina terminalis after complete tumor removal. The basilar artery (B) and the right posterior cerebral artery (P1) are observed through the broken TVF (asterisk). E2. Coronal MRI scan showing a large multilobulated CP (t) expanding from the sella to the third ventricle. The pituitary stalk is not visible and the hypothalamus is located at the mid-third portion of the tumor (red arrows).
5.5 The Mamillary Body Angle
Identification of the position and anatomical status of the whole TVF on conventional MRI studies from CP patients is quite difficult, particularly when CPs are larger than 3cm, because the infundibulum and tuber cinereum are severely distorted and they cannot usually be distinguished from the CP capsule. The compact structure of the mamillary bodies (MBs) makes these structures remain the only identifiable component of the TVF in many cases. Based on this observation, our group defined in 2013 the mammillary body angle (MBA) as a useful radiological tool to ascertain the position of the TVF regarding the tumor [62]. The MBA is defined as the angle formed by the intersection of the plane tangential to the base of the mammillary bodies with the plane tangential to the fourth ventricle floor (Figure 8). This angle can easily be measured on midsagittal MRI scans (Figure 6. A1-D1). In healthy individuals without intracranial pathology, the normal MBA value usually ranges between 50° and 70°. CP growth causes a progressive displacement and distortion of both the TVF and the MBs, and a change in the MBA value can be correlated with the TVF status, depending on the original site of tumor development along the pituitary-hypothalamus axis (Figure 8). Thus, this radiological sign has proven useful to predict CP topography. Tumors originated below the TVF at a sellar/suprasellar position typically cause an upward displacement of the mamillary bodies, shifting the MBA towards an obtuse value (>90°) (Figure 6. B1). An obtuse MBA is a strong predictor of the pseudointraventricular CP topography. By contrast, an acute MBA (<90°) is usually observed in intraventricular CPs displacing the TVF downwards as they expand within the 3V. The MBA value becomes even more reduced (hyperacute, <30°) in cases of CPs originating within the TVF itself (not-strictly intraventricular or infundibulotuberal CPs) (Figure 6. D1), as these tumors push the MBs against the midbrain while expanding within the tuber cinereum [62]. Consequently, a hyperacute MBA strongly suggests a severe CP-hypothalamic adhesion, usually between the central portion of the tumor and the remnants of the TVF.
Figure 8 The mamillary body angle (MBA) and its relation to craniopharyngioma topography. A: scheme illustrating how the MBA is measured on a midsagittal section. The MBA is formed by the intersection of the plane tangential to the base of the mamillary bodies (MBs) with the plane tangential to the floor of the fourth ventricle. Normal MBA ranges from 30º to 60º. B: Not-strictly intraventricular or infundibulotuberal CPs (t) developed in the TVF itself typically show hyperacute MBAs as the MBs are displaced towards the midbrain during tumor enlargement. C: Pseudointraventricular CPs (t) originated in the suprasellar cistern push the TVF upward towards the fornices and roof of the 3V leading to an increase in the MBA value (obtuse MBA).
5.6 Optic Chiasm Distortions
Visual impairment is one of the major and earliest presenting symptoms among CP patients. This deficit is due to the progressive distortion of the optic chiasm by the tumor. The direction and severity of optic chiasm distortion is mainly related to the original site of tumor development, and will significantly influence the severity and outcome of visual deficits. Our group systematically analyzed these distortions in a cohort of well described CP cases, and we were able to identify repetitive chiasm distortion patterns associated with specific tumor topographies [90]. The chiasm distortion types showed a strong correlation with the severity of visual deficits and their reversibility after tumor removal. Two major types of chiasm distortion could be identified on midsagittal MRI sections: compression and stretching (Figure 9). Compressed chiasms are characterized by a crescent and swollen appearance, a deformation that is typically caused by CPs originated within the TVF at the same level or slightly above the horizontal plane of the chiasm (Figure 9. B). In contrast, stretched chiasms show an elongated and thinned appearance after being pushed upwards by a tumor growing below or in front of the chiasm plane (Figure 9. C). In addition to the shape alteration, the optic chiasm may be displaced in a preferential direction by the tumor growth. Among the compressed chiasms, two major subgroups can be distinguished: i) chiasm compressed downward, when the chiasm is slightly pushed and displaced beneath the lower pole of the tumor (Figure 9. B1); ii) chiasm compressed forward, when the chiasm is displaced towards the tuberculum sellae and smashed against this bony structure (Figure 9. B2). Among stretched chiasms, three major displacements may occur: i) stretched forward, when the chiasm is elongated along the anterior margin of the tumor (Figure 9. C1); ii) stretched upward, when it is elongated over the tumor dome (Figure 9. C2); and, iii) stretched backward, when it is elongated along the posterior margin of the tumor (Figure 9. C3) [90].
The importance of identifying these optic chiasm distortion patterns on preoperative MRI scans is to assess their correlation with the presence and severity of specific visual deficits and with the postoperative visual outcome [90]. For example, vision is not impaired in 80% of CP patients whose optic chiasm shows a normal appearance or a downward compression. These cases also associate the best visual outcome. On the contrary, more than 80% of patients with either forward compressed or stretched distortions have visual deficits. The upward stretched pattern associates a rate of severe visual disturbances as high as 75%, as well as the worst visual outcome. About one third of CP patients with a chiasm stretched upward will not experience any visual improvement following tumor removal. This poor visual outcome is probably the result of an irreversible axonal degeneration caused by the effect of three simultaneous mechanical deformations: elongation of the fibers; compression of the optic nerves at the level of the sharp bone edges of the optic foramina; and strangulation of the dorsal surface of the chiasm by the anterior communicating artery complex (Figure 9. C). The type of optic chiasm distortion is also a valuable MRI sign to predict the CP topography [90]. Strictly intraventricular CPs typically do not cause any deformation to the optic chiasm (Figure 9. A1), or they only slightly compress it downwards (Figure 9. B1). On the contrary, the forward compressed distortion points to the not-strictly intraventricular category (Figure 9. B2), whereas chiasms stretched forward suggest a secondary intraventricular position (Figure 9. C1) and the upward stretched alteration is usually observed in the pseudointraventricular and sellar-suprasellar topographies (Figure 9. C2) [90].
Figure 9 Optic chiasm distortions caused by craniopharyngiomas as relate to tumor topography. The upper row shows schematic drawings of the three major types of chiasm distortions found in CP cases. The lower panels show midsagittal MRI scans of representative cases. A. Normal chiasm: a normal chiasm shape and position is typically found in tumors (t) with a strictly intraventricular topography (A1). B. Compressed chiasm: a chiasm with a swollen appearance is generally found in intraventricular-retrochiasmatic CPs (t) that push the chiasm towards the planum sphenoidale (arrows). The compressed distortion is subclassified into downward displaced chiasm at the antero-inferior margin of the tumor (B1), and forward displaced chiasm, pushing against the tuberculum sellae (B2). C. Stretched chiasm: elongation of the chiasm generally occurs with CPs (t) originated beneath the third ventricle floor. Arrows indicate the three mechanisms involved in damaging the optic fibers: i) compression of the optic nerves by the sharp bone edges of the optic foramina (grey arrows); ii) elongation of the chiasm (white arrows); and iii) strangulation of the chiasm dorsal surface by the A1-anterior communicating artery complex (black arrows). Three subgroups can be identified depending on the displacement direction: forward (C1); upward (C2); and backward (C3).
6. The Impact of Topography and Adherence on Craniopharyngioma Recurrence
Together with hypothalamic injury, CP recurrence represents a formidable challenge posed by these complex tumors. This is mainly due to the difficulty in predicting such recurrence, in addition to the high morbidity and mortality rates associated with surgery of recurrent tumors [91]. Moreover, the rate of patients affected by CP recurrence is rather high, as one third overall of these tumors recur after a 3-year postoperative interval. For these reasons, there has recently been a growing interest in using molecular changes present in CP cells as a potential tool to predict the likelihood of tumor recurrence [18]. Unfortunately, there is no agreement on the actual reliability of molecular alterations to predict CP recurrence. Lack of clear conclusions are probably due to the fact that most molecular studies have the shortcoming of analyzing the CP molecular profile without taking into consideration the individual type of treatment and pathological features of each tumor, among them CP topography and tumor adhesion pattern [18].
Most authors agree that an incomplete tumor removal is the major predictor of CP recurrence [91]. Apart from the surgeons’ skills, accurate CP topography and type of tumor adhesion are the major factors that will determine the possibility of achieving a complete tumor removal. A correct definition of these pathological factors must be established prior to any attempt at analyzing the impact of the molecular changes in CP recurrence. For example, it should be noted that the wide and strong adhesions to the surrounding brain observed in infundibulo-tuberal CPs, as well as the common microscopic finding of finger-like tumor protrusions into the hypothalamus that characterize this topography, are two causes explaining why tumor remnants can be left behind unintentionally even after an apparently gross total removal [4,91]. On the contrary, strictly intraventricular CPs, particularly those with a squamous papillary histology, are generally characterized by a clear and loose cleavage plane between the tumor and the hypothalamus, except at the point of a small pedicle/patch attachment to the TVF, that generally allows for a complete removal [5,6,34]. Thus, the molecular changes in these two topographical categories are not comparable, and a stratified analysis of the molecular alterations for each topography and degree of tumor removal is necessary.
7. CP Topography: The Fundamental Variable in Selecting a Surgical Approach
A wide range of surgical approaches have been employed for CPs, such as the pterional, subfrontal, transsphenoidal, transcallosal, frontal-trans-ventricular and interhemispheric. Overall, the surgeon’s experience and preference have normally dictated the particular chosen approach . Nevertheless, different CP topographies and adhesion patterns support the concept that certain routes are more suitable than others for specific CP-hypothalamus relationships. Therefore, an essential aspect of CP surgical planning is to decide “where to begin”. The optimal surgical route is that which provides a direct and broad view of the tumor-brain cleavage plane, particularly of the expected areas of maximal adhesion to the hypothalamus [1,33,42,49,55,58,84].
The upper trans-ventricular routes can only be used safely in strictly intraventricular CPs, as in these cases the hypothalamus is situated below the tumor (Figure 6. E2). These lesions typically present small attachments to the inner side of the TVF (Figure 7. B1) that can usually be released straightforwardly through a trasncallosal or frontal-transventricular approach [6,46,92,93]. However, these routes associate a high risk of iatrogenic hypothalamic injury when used to remove any of the remaining topographical CP categories involving the 3V [2,38,66,94]. The reason is that upper trans-ventricular approaches do not offer a direct view of the basal hypothalamus, the region to which most not-strictly intraventricular and secondary intraventricular CPs are strongly attached. The trans-lamina terminalis approach, either through a pterional, subfrontal or interhemispheric route, provides a direct view of the TVF the usual attachment site of CPs involving the 3V, and is therefore suitable to remove either strictly or not-strictly intraventricular tumors [5,6,31,46,92,95]. Some authors such as Yasargil and Steno favored the use of combined basal and upper approaches to have a complete view of the tumor-hypothalamus surface [2,49].
In the last ten years, the use of endoscopic endonasal transsphenoidal routes to remove CPs has been expanding [55,57,58]. The major advantage of this route is that it fully exposes the tumor-hypothalamus adhesion plane present in tumors developing within the infundibulum (infundibulo-tuberal CPs) and in suprasellar lesions invading the 3V (secondary-intraventricular CPs). Nevertheless, the advantage of performing a sharp dissection under direct view should be counterbalanced by the high risk of cerebrospinal fluid fistula due to the direct connection which will remain between the 3V and the nose, particularly when this approach is used by non-experts [96,97].
8. CP-Hypothalamus Adherence Severity: The Fundamental Factor in Deciding the Degree of Tumor Removal
The debate about the solid decision of tumor removal is still highly controversial among experts on CP treatment. Most neurosurgeons agree that a complete tumor resection is the optimal way of reducing the chances of tumor recurrence and the hazardous procedures for treating recurrent CPs, but many others advocate a conservative, incomplete removal to reduce the risk of hypothalamic damage and the long-term associated invalidating sequelae [66,98,99,100]. Nevertheless, we firmly believe that the decision regarding the degree of tumor removal should not be based on a specific technique or opinion but rather on the individual CP topography and its pattern of adherence. Thus, aside from the surgical approach, the second aspect of the surgical planning to be considered, is “when to stop”. An accurate preoperative definition of the risk of hypothalamic injury for each case is essential to take the proper decision about the degree of tumor removal most suitable. This aspect of surgical planning should also be part of patient counselling.
Conventional MRI studies can correctly identify the CPs presenting the most severe adhesions to the hypothalamus (levels IV and V) in approximately 90% of cases [9]. The MRI signs that best predict hypothalamic adherence with a high surgical risk are the position of the hypothalamus around the mid-third of the tumor, the amputation of the pituitary stalk and an elliptical tumor shape. In most of these cases a radical removal would inevitably lead to irreversible hypothalamic injury, and therefore an incomplete tumor removal is strongly advocated.
9. Conclusions
The widespread, inaccurate use of the term “suprasellar” to define CP topography should be abandoned and replaced by an accurate definition in each case. Most CPs actually involve the 3V, and a rate as high as 40% originate in the infundibulum or tuber cinereum, growing in close contact with the hypothalamus. An accurate definition of tumor position is the fundamental first step in planning a proper surgical treatment. Likewise, a generalized treatment policy for CPs is not valid nowadays. CP heterogeneity regarding tumor location and adhesion to adjacent structures support a tailored treatment based on a careful preoperative MRI assessment of topography and CP-brain relationships. CP topography and the pattern of CP-hypothalamus adhesions expected to be found during the surgical procedure can be reliably predicted with conventional MRI studies in most cases. The highest risk of hypothalamic injury during surgical removal is associated with tumors originated within the TVF itself (infundibulo-tuberal or not-strictly intraventricular CPs) or in suprasellar lesions that have eventually invaded the 3V (secondary-intraventricular CPs). These two CP categories are characterized by a direct contact between the tumor tissue and the hypothalamus without any intervening meningeal layer to be used as a safe dissection plane. In these cases, in which the hypothalamus is usually positioned around the mid-third or central region of the tumor and the pituitary stalk has an amputated appearance on preoperative MRI, an incomplete tumor removal is strongly recommended to avoid iatrogenic hypothalamic injury.
Acknowledgments
We especially thank Crystal Smith and Liliya Gusakova, reference librarians at the National Library of Medicine, NIH (Bethesda, MD), for their kind assistance during the process of searching and retrieving articles and monographs used in this study. We are indebted to Bill Landis and all the staff of the Manuscripts and Archives Department of the Sterling Memorial Library at Yale University (New Haven, CT) for their kind assistance in accessing the Cushing’s Brain Tumor Registry. We are also grateful to Melissa Grafe, librarian at the Medical History Library at Yale University (New Haven, CT) and Jack Eckert and the staff at the Francis Countway Medical Library at Harvard Medical School (Boston, MA) for their invaluable help in obtaining some of the original research used for this study. Finally, we are grateful to George Hamilton for his critical review of the language and style of the manuscript.
Author Contributions
Conception and design: Prieto and Pascual. Acquisition of data: Prieto and Pascual. Drafting the article: Prieto and Pascual. Critically revising the article: Prieto and Pascual.
Funding
This project did not obtain any financial support from a sponsor or research grant.
Competing Interests
The authors have declared that no competing interests exist.
References
- Steno J. Microsurgical topography of craniopharyngiomas. Acta Neurochir Suppl. 1985; 35: 94–100. [CrossRef]
- Steno J, Malácek M, Bïzik I. Tumor-third ventricular relationships in supradiaphragmatic craniopharyngiomas: correlation of morphological, magnetic resonance imaging, and operative findings. Neurosurgery. 2004; 54: 1051-1058 [CrossRef]
- Pascual JM, Carrasco R, Prieto R, González-Llanos F, Alvarez F, Roda JM. Craniopharyngioma classification. J Neurosurg. 2008; 109: 1180-1182. [CrossRef]
- Pascual JM, Prieto R, Carrasco R. Infundibulo-tuberal or not strictly intraventricular craniopharyngioma: evidence for a major topographical category. Acta Neurochir (Wien). 2011; 153: 2403–2426. [CrossRef]
- Pan J, Qi S, Lu Y, Fan J, Zhang X, Zhou J, et al. Intraventricular craniopharyngioma: morphological analysis and outcome evaluation of 17 cases. Acta Neurochir (Wien). 2011; 153: 773-784. [CrossRef]
- Pascual JM, Gonzalez-Llanos F, Barrios L, Roda JM. Intraventricular craniopharyngiomas: Topographical classification and surgical approach selection based on an extensive overview. Acta Neurochir (Wien). 2004; 146: 785–802. [CrossRef]
- Prieto R, Pascual JM, Rosdolsky M, Castro-Dufourny I, Carrasco R, Strauss S, et al. Craniopharyngioma adherence: a comprehensive topographical categorization and outcome-related risk stratification model based on the methodical examination of 500 tumors. Neurosurg Focus. 2016; 41: E13. [CrossRef]
- Prieto R, Pascual JM, Barrios L. Topographic diagnosis of craniopharyngiomas: The accuracy of MRI findings observed on conventional T1 and T2 images. AJNR Am J Neuroradiol. 2017; 38: 2073-2080. [CrossRef]
- Prieto R, Pascual JM, Rosdolsky M, Barrios L. Preoperative Assessment of Craniopharyngioma Adherence: Magnetic Resonance Imaging Findings Correlated with the Severity of Tumor Attachment to the Hypothalamus. World Neurosurg. 2018; 110: e404-e426. [CrossRef]
- Prieto R, Pascual JM, Rosdolsky M, Barrios L. Preoperative Assessment of Craniopharyngioma Adherence: Magnetic Resonance Imaging Findings Correlated with the Severity of Tumor Attachment to the Hypothalamus. World Neurosurg. 2018; 110: e404-e426. [CrossRef]
- Pascual JM, Prieto R, Mazzarello P. Sir Victor Horsley: Pioneer craniopharyngioma surgeon. J Neurosurg. 2015; 123: 39-51. [CrossRef]
- Pascual JM, Prieto R. Harvey Cushing and pituitary case number 3 (Mary D.): the origin of this most baffling problem in neurosurgery. Neurosurg Focus. 2016; 41: E6. [CrossRef]
- Boyce R, Beadles CF. A further contribution to the study of the pathology of the hypophysis cerebri. J Pathol Bacteriol. 1893; 1: 359–383. [CrossRef]
- Erdehim J. Über Hypophysengangsgeschwülste und Hirncholesteatome. Sitzungsb Kais AkadWissen Math NaturwKlin. 1904; 113: 537–726.
- Benda C. Beiträgezurnormalen und pathologischenHistologie der menschlichen Hypophysis cerebri. Berl Klin Wochnschr. 1900; 37:1205–1210
- Pascual JM, Rosdolsky M, Prieto R, StrauS, Winter E, Ulrich W. Jakob Erdheim (1874–1937): father of hypophyseal-duct tumors (craniopharyngiomas). Virchows Arch. 2015; 467: 459–469. [CrossRef]
- Pascual JM, Prieto R, Rosdolsky M, Strauss S, Castro-Dufourny I, Hofecker V, et al. Cystic tumors of the pituitary infundibulum: seminal autopsy specimens (1899 to 1904) that allowed clinical-pathological craniopharyngioma characterization. Pituitary. 2018; 21: 393-405. [CrossRef]
- Prieto R, Pascual JM. Can tissue biomarkers reliably predict the biological behavior of craniopharyngiomas? A comprehensive overview. Pituitary. 2018; 21: 431-442. [CrossRef]
- Apps JR, Carreno G, Gonzalez-Meljem JM, Haston S, Guiho R, Cooper JE, et al. Tumour compartment transcriptomics demonstrates the activation of inflammatory and odontogenic programmes in human adamantinomatous craniopharyngioma and identifies the MAPK/ERK pathway as a novel therapeutic target. Acta Neuropathol. 2018; 135: 757-777. [CrossRef]
- Buslei R, Rushing EJ, Giangaspero F, Paulus W, Buger PC, Santaga S. Craniopharyngiomas. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK (eds). WHO classification of tumors of the central nervous system. 4th ed. Lyon: IARC Press. 2016; 324–329.
- Lopes MBS. The 2017 World Health Organization classification of tumors of the pituitary gland: a summary. Acta Neuropathol. 2017; 134: 521-535. [CrossRef]
- Babinski J. Tumeur du corps pituitaire sans acromégalie et avec arrêt de développement des organes génitaux. Rev Neurol. 1900; 8: 531–533.
- Fröhlich A. Ein fall von tumor der hypophysis cerebri ohne akromegalie. Wien Klin Rundschau. 1901; 15: 883–886. 906–908.
- Castro-Dufourny I, Carrasco R, Prieto R, Pascual JM. Jean Camus and Gustave Roussy: pioneering French researchers on the endocrine functions of the hypothalamus. Pituitary. 2017; 20: 409–421. [CrossRef]
- Pascual JM, Prieto R, Barrios L. Harvey Cushing's craniopharyngioma treatment: Part 1. Identification and clinicopathological characterization of this challenging pituitary tumor. J Neurosurg. 2018. DOI: https://doi.org/10.3171/2018.5.JNS18153
- Cushing H. Congenital tumors: the craniopharyngiomas. In: Intracranial Tumors. Notes upon a series of two thousand verified cases with surgical-mortality percentages pertaining thereto. Springfield, IL: Charles C Thomas. 1932; 93–104.
- Osborn AG, Salzman KL, Barkovich AJ. Diagnostic Imaging. Brain. 2nd Ed. Friesens, Canada: AmirsysInc; 2010; Section II-2: p 32-35.
- Alalade AF, Ogando-Rivas E, Boatey J, Souweidane MM, Anand VK, Geefield JP, et al. Suprasellar and recurrent pediatric craniopharyngioma: expanding indications for the extended endoscopic transsphenoidal approach. J Neurosurg Pediatr. 2018; 21: 72-80. [CrossRef]
- Bailey P. Craniopharyngiomas. Syndrome of the hypothalamus. In: Intracranial Tumors. Springfield, IL: Charles C. Thomas. 1933; 113-137.
- Le Gros Clark WE, Beattie J, Riddoch G, et al (eds). The Hypothalamus: Morphological, Functional, Clinical and Surgical Aspects. Edinburgh: Oliver and Boyd. 1938.
- Prieto R, Pascual JM. Norman M. Dott, master of hypothalamic craniopharyngioma surgery: the decisive mentoring of Harvery Cushing and Percival Bailey at Peter Bent Brigham Hospital. J Neurosurg. 2017; 127: 927-940. [CrossRef]
- Northfield DWC. Rathke-pouch tumours. Brain. 1957; 80: 293–312. [CrossRef]
- Qi S, Lu Y, Pan J, Zhang X, Long H, Fan J. Anatomic relations of the arachnoidea around the pituitary stalk: relevance for surgical removal of craniopharyngiomas. Acta Neurochir (Wien). 2011; 153: 785–796. [CrossRef]
- Qi S, Pan J, Lu Y. Craniopharyngiomas - Classification and surgical treatment. Frontiers in Neurosurgery, Vol. 4. Sharjah, UAE: Bentham Science Publishers. 2017.
- RougerieJ, Fardeau M. Les cranio-pharyngiomes. Paris: Masson et Cie Editeurs; 1962.
- Rougerie J. What can be expected from surgical treatment of craniopharyngiomas in children. Report of 92 cases. Childs Brain. 1979; 5:433–449.
- Pertuiset B, Janny P, Allègre G, Olivier L. Cranio-pharyngiomes simulant une tumeur antérieure du iii ventricule. Presse Med. 1962; 70: 1846–1848.
- Pertuiset B. Craniopharyngiomas. En: Vinken PJ, Bruin GW, editores. Handbook of Clinical Neurology. Vol. 19, Part II: Tumors of the brain and skull. Amsterdam: North Holland Publishing Company. 1975; 531–572.
- Hoffman HJ, Hendrick EB, Humphreys RP, Buncic JR, Armstrong DL, Jenkin RD. Management of craniopharyngioma in children. J Neurosurg. 1977; 47: 218–227. [CrossRef]
- Hoffman HJ, De Silva M, Humphreys RP, Drake JM, Smith ML, Blasser SI. Aggressive surgical management of craniopharyngiomas in children. J Neurosurg. 1992; 76: 47-52. [CrossRef]
- Konovalov AN. Operative management of craniopharyngiomas. Adv Tech Stand Neurosurg. 1981; 8: 281–318. [CrossRef]
- Konovalov AN, Gorelyshev SK. Surgical treatment of anterior third ventricle tumours. Acta Neurochir (Wien). 1992; 118: 33–39. [CrossRef]
- Konovalov AN, Kalini PL, Kutini MA, Fomichev DV, Kadashev BA, Astafyeva LI, et al. Transphenoidal surgery of cranioharyngiomas: from palliative surgeries to radical removal. N NBurdenko J Neurosurg. 2013; 77: 3-12
- Sweet WH. Craniopharyngiomas, with a note on Rathke’s cleft or epithelial cyst and on suprasellar cysts. In: Schmideck HH, Sweet WH (eds). Operative neurosurgical techniques, indications, methods and results. 2nd ed. New York: Grune&Stratton. 1988; 291–325.
- Maira G, Anile C, Rossi GF, Colosimo C. Surgical treatment of craniopharyngiomas: An evaluation of the transsphenoidal and pterional approaches. Neurosurgery. 1995; 36: 715–724. [CrossRef]
- Maira G, Anile C, Colosimo C, Cabezas D. Craniopharyngiomas of the third ventricle: Trans-lamina terminalis approach. Neurosurgery. 2000; 47: 857–865. [CrossRef]
- MairaG, Anile C, Albanese A, Cabezas D, Pardi F, Vignati A. The role of transsphenoidal surgery in the treatment of craniopharyngiomas. J Neurosurg. 2004; 100: 445-451. [CrossRef]
- Samii M, Tatagiba M. Craniopharyngioma. In: Kaye AH, Laws Jr ER (eds). Brain tumors. London: Churchill Livingstone. 1995; 873–894.
- Yasargil MG. Craniopharyngioma. In: Microneurosurgery. Vol IV-B, Microneurosurgery of CNS tumors. Sttutgart-New York: Georg Thieme Verlag. 1996; 205–223.
- Fahlbusch R, Honegger J, Paulus W, Huk W, Buchfelder M. Surgical treatment of craniopharyngiomas: Experience with 168 patients. J Neurosurg. 1999; 90: 237–250. [CrossRef]
- Hofmann BM, Höllig A, Strauss C, Buslei R, Buchfelder M, Fahlbusch R. Results after treatment of craniopharyngiomas: Further experiences with 73 patients since 1997. J Neurosurg. 2012; 116: 373–384. [CrossRef]
- Tomita T, Bowman RM. Craniopharyngiomas in children: Surgical experience at children’s memorial hospital. Childs Nerv Syst. 2005; 21: 729–746. [CrossRef]
- Shi XE, Wu B, Zhou ZQ, Fan T, Zhang YL. Microsurgical treatment of craniopharyngiomas: Report of 284 patients. Chin Med J (Engl). 2006; 119: 1653–1663.
- Shi XE, Wu B, Zhou ZQ, Fan T, Zhang YL. Craniopharyngioma: Surgical experience of 309 cases in China. Clin Neurol Neurosurg. 2008; 110: 151–159. [CrossRef]
- Kassam AM, Gardner PA, Snyderman CH, Carrau RL, Mintz AH, Prevedello DM. Expanded endonasal approach, a fully endoscopic transnasal approach for the resection of midline suprasellar craniopharyngiomas: A new classification based on the infundibulum. J Neurosurg. 2008; 108: 715–728. [CrossRef]
- Mortini P, Losa M, Pozzobon G, Barzaghi R, Riva M, Acerno S, et al. Neurosurgical treatment of craniopharyngioma in adults and children: early and long-term results in a large case series. J Neurosurg. 2011; 114: 1350-1359. [CrossRef]
- Cavallo LM, Solari D, Esposito F, Cappabianca P. The endoscopic endonasal approach for the management of craniopharyngiomas involving the third ventricle. Neurosurg Rev. 2013; 36: 27-37. [CrossRef]
- Tang B, Xie SH, Xiao LM, Huang GL, Wang ZG, Yang L, et al. A novel endoscopic classification for craniopharyngioma based on its origin. Sci Rep. 2018; 5: 10215. [CrossRef]
- Northfield DWC. The surgery of the central nervous system. London: Blackwell Scientific Publications. 1973; 280–330.
- Wang KC, Kim SK, Choe G, Chi JG, Cho BK. Growth patterns of craniopharyngioma in children: Role of the diaphragm sellae and its surgical implication. Surg Neurol. 2002; 57: 25–33. [CrossRef]
- Wang KC, Kim SK, Hong SH, Cho BK. Origin of craniopharyngiomas: Implication on the grow pattern. Childs Nerv Syst. 2005; 21: 628–34. [CrossRef]
- Pascual JM, Prieto R, Carrasco R, Barrios L. Displacement of mammillary bodies by craniopharyngiomas involving the third ventricle: surgical-MRI correlation and use in topographical diagnosis. J Neurosurg. 2013; 119: 381–405. [CrossRef]
- Ciric IS, Cozzens JW. Craniopharyngiomas: Transsphenoidal method of approach–For the virtuoso only? Clin Neurosurg. 1980; 27: 169–87. [CrossRef]
- Raybaud C, Rabehanta P, Girard N. Aspects radiologiques des craniopharyngiomes. Neurochirurgie. 1991; 37: 44–58.
- De Vile CJ, Grant DB, Kendall BE, Neville BGR, Stanhope R, Watkins KE, Hayward RD. Management of childhood craniopharyngioma: can the morbidity of radical surgery be predicted? J Neurosurg. 1996; 85: 73-81. [CrossRef]
- Sainte-Rose C, Puget S, Wray A, Zerah M, Grill J, Brauner R, et al. Craniopharyngioma: The pendulum of surgical management. Childs Nerv Syst. 2005; 21: 691–695. [CrossRef]
- Puget S, Garnett M, Wray A, Grill J, Habrand JL, Bodaert N, et al. Pediatric craniopharyngiomas: Classification and treatment according to the degree of hypothalamic involvement. J Neurosurg. 2007; 106: 3–12. [CrossRef]
- Zhang YQ, Wang CC, Ma ZY. Pediatric craniopharyngiomas: Clinicomorphological study of 189 cases. Pediatr Neurosurg. 2002; 36: 80–84. [CrossRef]
- Zhang YQ, Ma ZY, Wu ZB, Luo SQ, Wang ZC. Radical resection of 202 pediatric craniopharyngiomas with special reference to the surgical approaches and hypothalamic protection. Pediatr Neurosurg. 2008; 44: 435–443. [CrossRef]
- Pascual JM, Prieto R, Carrasco R, Castro-Dufourny I, Strauss S, Gil-Simoes R, et al. Premio Sixto Obrador 2013. Modelo topográfico de 3 ejes para el tratamiento quirúrgico de los craneofaringiomas. Parte I: Evolución histórica del diagnóstico topográfico y métodos de clasificación de los craneofaringiomas. Neurocirugia (Astur). 2014; 25: 154-169. [CrossRef]
- Pascual JM, Prieto R, Carrasco R, Castro-Dufourny I, Strauss S, Gil-Simoes R, et al. Neurocirugia (Astur). Premio Sixto Obrador 2013. Modelo topográfico de 3 ejes para el tratamiento quirúrgico de los craneofaringiomas. Parte II: Evidencias anatómicas y neurorradiológicas que definen el modelo de clasificación de 3 ejes y su utilidad para predecir el riesgo quirúrgico individual. 2014; 25: 211-239.
- Kobayashi T, Kageyama N, Yoshida J, Shibuya N, Yonezawa T. Pathological and clinical basis of the indications for treatment of craniopharyngiomas. Neurol Med Chir (Tokyo). 1981; 21: 39–47. [CrossRef]
- Kubota T, Yamamoto S, Kohno H, Ito H, Hayashi M. Operative procedures of craniopharyngiomas estimated by autopsy findings. Neurol Med Chir (Tokyo). 1980; 20: 341–354. [CrossRef]
- Zülch KJ. Atlas of Gross Neurosurgical Pathology. New York: Springer-Verlag; 1975, p. 155–160. [CrossRef]
- Ben-Shlomo A, Melmed S. Hypothalamic regulation of anterior pituitary function. In: Melmed S (ed): The Pituitary. 3rd ed. Amsterdan: Academic Press, Elsevier. 2011; 21-45.
- Prieto R, Pascual JM, Castro-Dufourny I, Carrasco R, Barrios L. Craniopharyngioma: Surgical Outcome as Related to the Degree of Hypothalamic Involvement. World Neurosurg. 2017; 104: 1006-1010. [CrossRef]
- Cushing H. Papers relating to the pituitary body, hypothalamus and parasympathetic nervous system. Baltimore: Charles C Thomas. 1932.
- Swaab D. The human hypothalamus. Basic and clinical aspects. In: Aminoss MJ, Boller S, Swaab D (eds) Handbook of clinical neurology, vol 79 part 1 (3rd series, vol 1). Amsterdam: Elsevier. 2012; 243–248
- Clarke IJ, Campbell R, Smith JT, Prevot V, Wray S. Neuroendocrine control of reproduction. In: Fink G, Pfaff DW, Levine JE (eds) Handbook of neuroendocrinology. London: Academic Press, Elsevier Inc. 2012; 197–236. [CrossRef]
- Young JK: Hunger, Thirst, Sex and Sleep: How the Brain controlsour passions. Plymouth, UK: Rowman & Littlefield Publishers Inc. 2012.
- Young JK, Polston EK. Specialized features of the Arcuate Nucleus of the hypothalamus. In: Duda ´s B (ed) The Human Hypothalamus: Anatomy, functions and disorders. New York : Nova Science Publishers. 2013.
- Castro-duforny I, Carrasco R, Prieto R, Pascual JM. Infundibulo-tuberal syndrome: the origins of clinical neuroendocrinology in France. Pituitary. 2015; 18: 838-843. [CrossRef]
- Critchley M, Ironside RN. The pituitary adamantinoma. Brain. 1926; 49: 437-481. [CrossRef]
- Sweet WH. Radical surgical treatment of craniopharyngioma. Clin Neurosurg. 1976; 23: 52–79. [CrossRef]
- Khan EA, Gosch HH, Seeger J, Hicks JF. Forty-five years experience with craniopharyngiomas. Surg Neurol. 1973; 1: 5–12.
- Petito CK, DeGirolami U, Earle KM. Craniopharyngiomas: A clinical and pathological review. Cancer. 1976; 37: 1944–52. [CrossRef]
- Shillito Jr J. Craniopharyngiomas: The subfrontal approach, or none at all? Clin Neurosurg. 1980; 27: 188–205. [CrossRef]
- Prieto R, Pascual JM, Hofecker V, Winter E, Castro-Dufourny I, Carrasco R, et al. Craniopharyngioma adherence: a reappraisal of the evidence. Neurosurg Rev. 2018; 24. doi: 10.1007/s10143-018-1010-9. [CrossRef]
- Rossi A, Cama A, Consales A, Gandolfo C, Garrè ML, Milanaccio C, et al. Neuroimaging of pediatric craniopharyngiomas: a pictorial essay. J Ped Endocrinol Metab. 2006; 19: 299-319.
- Prieto R, Pascual JM, Barrios L. Optic chiasm distortions caused by craniopharyngiomas: clinical and magnetic resonance imaging correlation and influence on visual outcome. World Neurosurg. 2015; 83: 500-529. [CrossRef]
- Prieto R, Pascual JM, Subhi-Issa I, Jorquera M, Yus M, Martínez R. Predictive factors for craniopharyngioma recurrence: a systematic review and illustrative case report of a rapid recurrence. World Neurosurg. 2013; 79: 733-749. [CrossRef]
- King TT. Removal of intraventricular craniopharyngiomas through the lamina terminalis. Acta Neurochir (Wien). 1979; 45: 277-286. [CrossRef]
- Pascual JM, Prieto R, Castro-Dufourny I, Gil Simoes R, Carrasco R. Craniopharyngiomas of the third ventricle: topographical concepts of surgical interest.Br J Neurosurg. 2013; 27: 268-269. [CrossRef]
- Van Den Bergh R, Brucher JM. L’abord transventriculaire dans les crânio-pharyngiomes du troisièmeventricule. Apects neuro-chirurgicaux et neuro-pathologiques. Neurochirurgie. 1979; 16: 51-65.
- Prieto R, Pascual JM, Barrios L. Harvey Cushing's craniopharyngioma treatment: Part 2. Surgical strategies and results of his pioneering series. J Neurosurg. 2018. DOI: https://doi.org/10.3171/2018.5.JNS18154
- Koutourousiou M, Gardner PA, Fernandez-Miranda JC, Tyler-Kabara EC, Wang EW, Snydeman CH. Endoscopic endonasal surgery for craniopharyngiomas: surgical outcome in 64 patients. J Neurosurg. 2013; 119: 1194-1207 [CrossRef]
- Leng LZ, Greenfield JP, Souweidane MM, Anand VK, Schwartz TH. Endoscopic, endonasal resection of craniopharyngiomas: analysis of outcome including extent of resection, cerebrospinal fluid leak, return to preoperative productivity, and body mass index. Neurosurgery. 2012; 70; 110-123. [CrossRef]
- Meuric S, Brauner R, Trivin C, Souberbielle JC, Zerah M, Sainte-Rose C. Influence of tumor location on the presentation evolution of craniopharyngiomas. J Neurosurg. 2005; 103: 421-426. [CrossRef]
- Müller HL. Craniopharyngioma. Endocr Rev. 2014; 35: 513-543. [CrossRef]
- Müller HL, Merchant TE, Puget S, Martinez-Barbera JP. New outlook on the diagnosis, treatment and follow-up of childhood-onset craniopharyngioma. Nat Rev Endocrinol. 2017; 13: 299-312. [CrossRef]
