

Implementation of a Geriatric Patient-Centered Medical Home: the Geriatric Patient – Aligned Care Team (GeriPACT)
James S. Powers 1, 3, *![]() , Catherine Xie 1
, Catherine Xie 1![]() , Michelle Moseley 2
, Michelle Moseley 2![]() , Lovely Abraham 2
, Lovely Abraham 2![]() , Jennifer Buckner 2
, Jennifer Buckner 2![]() , Nkechi Azubike 2
, Nkechi Azubike 2![]()
- Vanderbilt University School of Medicine, Nashville, Tennessee, USA
- Tennessee Valley Healthcare System, Nashville, Tennessee, USA
- Geriatric Research Education and Clinical Center, Nashville, Tennessee, USA
* Correspondence: James S. Powers ![]()
Academic Editor: Michael Fossel
Received: May 21, 2018 | Accepted: August 3, 2018 | Published: August 13, 2018
OBM Geriatrics 2018, Volume 2, Issue 3 doi:10.21926/obm.geriatr.1803008
Recommended citation: Powers JS, Xie C, Moseley M, Abraham L, Buckner J, Azubike N. Implementation of a Geriatric Patient-Centered Medical Home: the Geriatric Patient – Aligned Care Team (GeriPACT). OBM Geriatrics 2018;2(3):008; doi:10.21926/obm.geriatr.1803008.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
Background: A Veterans Health Administration (VHA) patient centered medical home, the Geriatric Patient- Aligned Care Team (GeriPACT). Methods: Plan-Do-Study-Act (PDSA) cycles regarding strategy, resource development, patient and caregiver experience of care, and clinical care process improvement. Stakeholder engagement for half-time operation with initial grant support for personnel who also had collateral duties. Tracking of operations data. Results: The clinic population grew from 200 to 627 over a 7-year period. GeriPACT patients were frail with multiple co-morbidities, including a mean age 84, a 19.4% yearly hospitalization rate, and 12.2% died yearly. Collaborative team management of these complex patients reduced mean number of outpatient medications from 11 to 9, and the 30-day rehospitalization rate was 10%, approximately half the facility’s rate. Estimated yearly cost avoidance for GeriPACT was 1,963,243. Implementation of GeriPACT is impacted by limited availability of trained providers. Conclusions: GeriPACT may be a cost-effective way to manage high-risk, high-need elderly patients. GeriPACT expansion and implementation in all facilities has been made part of the VHA regional strategic plan.
Keywords
Implementation; medical model; patient-centered medical home
1. Background
The patient centered medical home (PCMH) model is being implemented by a growing number of health organizations in order to provide improved population health management: more comprehensive, coordinated, and patient-centered care [1]. The PCMH model includes team- based care focused on enhanced access and coordination. Published evaluations of the PCMH model in both large healthcare systems and individual practices have shown mixed results, with some studies demonstrating small positive effects on patient experiences and small to moderate positive effects on health care delivery [2,3,4]. In 2010 the Veterans Health Administration (VHA) implemented the PCMH model (Patient-Aligned Care Teams – PACT) in all primary care clinics, encompassing a population of 5 million veterans [5]. A 3-year implementation experience with PACT demonstrated a 3.0 staff per 1.0 primary care provider (PCP) ratio, a 20% reduction in return visits increasing new patient capacity, and a 10-fold increase in telephone care [6]. Over 50% of veterans receiving primary care are over age 65, with veterans over age 85 representing the fastest growing subpopulation. These older veterans represent some of the most cognitively and physically disabled high-risk, high-need patients of the VA patient population. The VA has supported a broad array of home and community-based services including both medical and personal care programs, to support the mission of the VHA Office of Geriatrics and Extended Care (GEC): access, balance, and coordination of care [7]. GeriPACT is an integral component of this initiative, a special population PACT initiated in 2011 for complex geriatric and other high-risk vulnerable veterans, providing integrated, interdisciplinary assessment and longitudinal management and coordination of both VA and non-VA services for patients and caregivers [8,9]. Little research has been done on the effectiveness of the PCMH for older adults, though there have been numerous proposed benefits [10].
2. Context and Development of the GeriPACT Model
The Tennessee Valley Healthcare System (TVHS) consists of two campuses, Nashville and Murfreesboro, and is located in Veterans Integrated Service Area (VISN) 9 in Southeast US. The Tennessee Valley Healthcare System (TVHS) is an integrated health care system in middle Tennessee comprised of 2 medical centers located 40 miles apart, and 12 community-based outpatient clinics. TVHS provides ambulatory care, primary care, a full range of specialized medical services in acute medicine and surgery, as well as a full range of extended care and mental health services. The patient population includes over 98,000 individuals of which approximately 97% are paneled in primary care. A market analysis showed that the Nashville campus of TVHS had a census of over 1000 patients greater than age 80, 35% of whom were rural or highly rural. The wait list for geriatric primary care was greater than 60 veterans, and the clinic also received many requests for geriatric evaluations, as well as falls and dementia consults. GeriPACT was developed from a small geriatric evaluation and management clinic that had been operating for 20 years, sharing space through a cooperative arrangement with the neurology and psychiatry outpatient clinics. VA transformational grant funding was available starting in 2011 for four years to cover 50% of the cost of increased staffing, and was essential in obtaining leadership approval to initiate GeriPACT at the Nashville campus [11,12].
The GeriPACT team consists of the GeriPACT provider (a 1 FTEE geriatrician or geriatric nurse practitioner with an outpatient panel size goal of approximately 800), social worker, clinical pharmacist, registered nurse care manager, licensed practical nurse, and medical clerical support assistant (all 1 FTEE staff). Additional staff including clinical psychologists and dietitians were shared with other primary care teams and consulted on a case-by-case basis. All providers were experienced in working as a coordinated unit delivering patient-centered assessments and managing medically complex and vulnerable elderly individuals (Figure 1). Patients and caregivers received frequent communications from the GeriPACT team, including contact when patients were hospitalized and following patient discharge from hospital and long-term care facilities.
We provide an evaluation of our innovative 7-year (2011-2018) GeriPACT regional experience with this team based care model, with reference to a framework for implementation research.
Geriatric Patient-Centered Medical Home
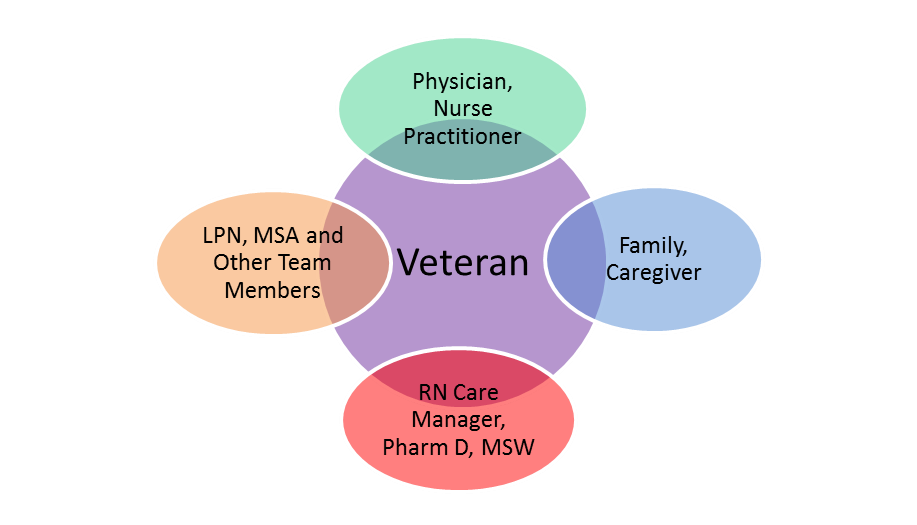
Figure 1 Structure of the PCMH concept as used in GeriPACT. Patients and their families/caregivers interact with a team of providers, including physicians, nurse practitioners, nurse care managers, social workers, licensed practical nurse (LPN), clinical pharmacists, medical support assistants (MSA), and other staff, all of whom work as a coordinated unit. Other staff including clinical psychologists and dietitians were shared with other primary care teams and consulted on a case-by-case basis.
3. Methods and Process Improvement Implementation of the Model
Planning for GeriPACT began in 2010 with meetings of potential stakeholders and supporters which included primary care physicians, the Chief of Staff, and Chiefs of Social Work and Pharmacy. Frequent quality improvement Plan-Do-Study-Act (PDSA) cycles regarding strategy, resource development, patient experience of care, and clinical care process improvement were performed. These exercises helped to identify key operational steps to enable full implementation of the PCMH. Three major attributes of the PCMH framed the PDSA cycles: access (same-day appointments, shared medical appointments, and non-appointment care), care management and coordination (focus on personalized care for high-risk high-need patients, chronic disease management, improved transitions between levels of care, and caregiver support), and practice redesign (defining team member roles, communication, and improved processes of work for visit as well as non-visit work). Analyzing the results and refining the change led to additional PDSA cycles. An initial interdisciplinary teamlet [13] was identified, consisting of the physician, registered nurse care manager care manager, licensed practical nurse, clinical pharmacist, social worker, and nurse practitioner. GeriPACT replaced an existing geriatric clinic that formerly cared for a primary care population of 200 older veterans. The team met with primary care providers at the facility to discuss referral processes, and population metrics were reviewed to identify potential patients to be invited to GeriPACT, including patients with age greater than 80, poor functional status, and advanced disease processes.
A strategy to obtain support and administrative buy-in for a part-time clinic was aided by VA transformational funding for a portion of the increased staffing essential to PCMH function. All clinic personnel had collateral duties and the physician director covered messages and patient care needs between clinic sessions. Not every patient needed to see each team member at every visit. The team became skilled in providing just-in-time (real-time, as needed) interdisciplinary consultation with colleagues engaged with individual patients. Frequent team meetings helped to develop interdisciplinary team function, facilitated workflow, and identify resource needs.
Operations data was reviewed during team meetings and utilized as a vehicle to promote quality improvement activities impacting the patient experience of care including caregiver support, waiting times, development of electronic consult protocols, and electronic health record (EHR) documentation.
GeriPACT operations data, consisting of population health and outcome metrics, were tracked utilizing the Veterans Information System Health and Technology Architecture (VISTA), as well as EHR provider panel management tools. Metrics tracked included patient age, numbers of medications, major diagnoses, hospitalizations, deaths, and clinic panel size. Data was collected continually during the development and implementation of the model, and summary statistics were conducted on an annual basis.
The Tennessee Valley Healthcare System Institutional Review Board determined this project as a quality improvement initiative.
4. Results
4.1 Outcome Data
Our GeriPACT panel proved to be a high-risk, high-need population with multiple comorbidities, as anticipated [9]. The mean patient age of the panel was 84 years, with 30 % having diabetes, 15% dementia and 12% congestive heart failure in addition to multiple other medical comorbidities, and an average 12% yearly mortality. Over the first four years of implementation, the GeriPACT team reduced yearly hospitalizations from 21% to 13% (mean 19%), the mean number of outpatient medications per patient fell from 11to 9, and the 30-day all cause readmission averaged 10% for this population of older adults (Table 1).
Table 1 GeriPACT Data (mean 2011-2016)
|
Population N=627 Mean Age |
84 |
|
Mean # outpatient medications |
8.7 |
|
Diagnoses CHF |
11.6% |
|
DM |
29.8% |
|
ASCVD |
28% |
|
Dementia |
14.6% |
|
Admitted |
19.4% |
|
30-day rehospitalization |
10% |
|
Expired |
12.2% |
Cost avoidance/year Rehospitalization 132,403*
Medication reduction 1,830,840**
1,963,243
*[compared to facility 30-day readmission 20%, 4.5 day hospitalization @ 10,885[14]]
**[mean reduction 2 medications/patient, 4/day cost avoidance per medication[15]]
Abbreviations: CHF (congestive heart failure), DM (diabetes mellitus), ASCVD (Atherosclerotic Cardiovascular Disease)
4.2 Successful Practices
Group appointments are scheduled so that patients can be seen by the physician as well as the pharmacist and/or social worker on the same day as needed. Additionally, the clinical pharmacist sees patients independently, focusing on polypharmacy and chronic disease (diabetes, hypertension, and chronic lung disease) medication management. The social worker also sees caregivers independently at times and responds to consultations concerning eligibility and obtainment of community-based services. The RN care coordinator utilizes the EHR dashboard (a snapshot of the patient panel providing current status, location, and pertinent clinical reminders) to identify and refer high-risk patients, including those with post-discharge acute care sensitive conditions, recent hospital and post-acute care discharges, and anticoagulation management needs.
4.3 Example of a group appointment
One of the clinic’s favorite patients is a 106 year-old veteran who still lives in his own apartment, albeit with the frequent assistance of his 86-year-old daughter. On clinic appointment days, he is seen immediately on arrival with a thorough assessment of his health maintenance needs by the licensed practical nurse, who also addresses all relevant clinical reminders in the VA EHR. The pharmacist performs a medication reconciliation, providing instruction and answering all questions posed by the patient and caregiver. The social worker assesses for any community-based care needs and for caregiver burden, utilizing a shared decision making process with discussion of available community resources. All team members communicate with the physician who examines the patient, provides advice and recommendations, and makes appropriate changes and referrals in the EHR. With each visit this centenarian obtains a teamlet consultation designed to maximize his person- centered care, providing access to a rich variety of skilled and nonskilled services, and assisting with caregiver burden.
4.4 Model Success Leads to Dissemination
The successful implementation of GeriPACT provided a helpful example in the early development of primary care PACT at our facility. VISN leadership became aware of GeriPACT outcomes and subsequently required GeriPACT development as part of the 2015 strategic plan at all regional facilities. The following year regional leadership further provided first year funding of approximately 3.5 million for all six facilities in the VISN 9 region to locally develop and fully implement the GeriPACT model throughout the region.
4.5 Barriers Along the Way
The TVHS GeriPACT clinic currently operates at 75% capacity. Provider recruitment and achievement of full staffing has been challenging, despite the cost effectiveness of the clinic based on cost avoidance methodology. Staff turnover is particularly challenging to maintaining optimal team function. Recruitment of providers and release of team members from collateral duties, including pharmacist coverage of medical specialties and social worker management of walk-in consultations, remain substantial barriers to implementation pending attainment of full workload. There continues to be efforts to fully staff Geri-PACT at all facilities in the region, with most clinics having achieved approximately 50% capacity over a 2– year period. Recruitment of trained providers, allocation of staffing with release from collateral duties, and achieving workload requirements during partial implementation remain challenges at all VISN 9 regional facilities.
5. Discussion and Implications
The GeriPACT model may be a value-added means to manage frail elderly patients, contributing to cost avoidance and improved patient outcomes. The clinic at the TVHS Nashville campus, functioning at approximately 75% capacity, realized an estimated 1,963,243 annual cost avoidance for the facility. We estimate that an enlarged GeriPACT capacity could realize even greater cost savings, based on economies of scale. Key initial cost avoidance domains include decreased outpatient medication and 30-day re-hospitalization rates. Several elements of transitional care described in literature as best practices can be found in the GeriPACT model: prompt post-discharge outpatient follow-up, open communication between providers, medication reconciliation and patient and/or caregiver education [16]. Furthermore, a team-based approach to transitional care is especially important for reducing readmissions, especially for the highest risk patients [17,18]. The GeriPACT model helps to ensure that relevant hospital records are obtained, medication changes are reviewed, and outpatient appointments are scheduled promptly to minimize wait times. Messaging systems are also available to patients, and post-discharge provider-patient communication is clear and comprehensive, resulting in best-possible transitions of care for vulnerable and high-risk patients [19,20,21]. While others have found lower utilization of inpatient and emergency services [2], and improved quality indicators [3] with the PCMH, detailed evaluation of long-term outcomes and downstream effects on healthcare utilization patterns remain ongoing endeavors at our facility.
Process improvement and transformational change takes time and requires organizational investment. The consolidated framework work for implementation research [22] suggests five elements of evaluation: intervention characteristics including core and adaptable components, outer setting consisting of external factors such as economic, political, or social contexts, inner setting consisting of the structure’s networks culture and readiness of the organization, participant characteristics including targeting users and other stakeholders who may be affected by the process of change, and the implementation process itself consisting of planned formal and informal activities, and intended and unintended actions to bring about change. In the development of GeriPACT at our facility, the interventions were data–driven and responded to input from key stakeholders including patients, clinicians, and administrators. Continued communication with stakeholders was crucial in providing continued support for the creation of GeriPACT. Implementation of GeriPACT occurred in the setting of an evolving VA primary care PCMH directive and with availability of partial grant support to offset staffing costs of the new clinic, in recognition of the large number of high-risk high-need elderly and their caregivers. The clinic was slowly expanded from a small existing clinic, utilizing collaborative staff and frequent team meetings to review quality and performance metrics (Table 2).
Table 2 Consolidated Framework for Implementation of GeriPACT. Includes core interventional characteristics, outer setting (external factors), inner setting (readiness of organizational structure), participant characteristic (stakeholders) and planned activities of the implementation process.
|
Constructs |
Model Demonstration |
|
Intervention characteristics |
Data-driven, constant stakeholder involvement |
|
Outer setting |
VA Primary Care PACT directive |
|
Inner setting |
Large number of high-risk, high-need elderly |
|
Participant characteristics |
Collaborative pilot practice |
|
Implementation process |
PDSA cycles, partial funding support |
Limitations: Recruitment of trained providers and allocation of staffing during partial implementation are challenges to GeriPACT development, especially given the national shortage of primary care and geriatric trained physicians [23-25], and full development of these clinics takes time. While medication reduction and reduced hospitalization are notable achievements of the model, we know little about other long-term benefits to the health system. The PCMH model was implemented in a non-fee-for-service system which placed a priority on cost avoidance, and thus the proposed staffing pattern inherent in the PCMH model may prove challenging for other payer systems in the private sector.
Replication and Future Plans: The GeriPACT operation involves a collaborative effort of many healthcare professionals. Risk assessment to identify high-risk high-need older patient populations being seen in other primary care and disease specific clinics for appropriate inclusion in GeriPACT, assisting colleagues with goals of care discussions, and expansion of model remain priorities. New EHR dashboard applications displaying specific GeriPACT panel comorbidities may be a helpful resource. GeriPACT personnel may also serve as effective resources for further support of high-risk, high-need elderly patient populations including consultation for dementia and caregiver support, and telehealth outreach for rural populations.
The high rate of multi-morbidity and mortality among these patients make GeriPACT an appropriate venue to expand primary palliative care services. The GeriPACT model is now being actively promoted nationally within the VA system, with evidence of adaptation to local context including variations in structural characteristics including staffing, allocation of clinical space, panel size, patient enrollment procedures, patient conditions managed, clinical services provided, and team composition. Future evaluation measures that are important in the development of the geriatric PCMH model includes further characterization of organizational contextual factors, staffing components, team function, provider satisfaction, patient and caregiver needs and satisfaction, patient reported outcomes, tracking of care transitions, and other performance and health outcomes metrics.
Author Contributions
Powers: Concept, design, analysis, interpretation, preparation of paperwork; Moseley, Buckner: Concept, design, preparation of paper; Xie, Abraham, Azubike: Preparation of paper.
Competing Interests
The authors have declared that no competing interests exist.
References
- Thomas S. Bodenheimer, Kevin Grumbach. Improving Primary Care: Strategies and Tools for a Better Practice. New York: McGraw-Hill Education / Medical, 2006.
- Cuellar A, Helmchen LA, Gimm G, Want J, Burla S, Kells BJ, et al. The CareFirst patient-centered medical home program: cost and utilization effects in its first three years. J Gen Intern Med. 2016; 31: 1382-1388. [CrossRef]
- Friedberg MW, Schneider EC, Rosenthal MB, Volpp KG, Werner RM. Association between participation in a multipayer medical home intervention and changes in quality, utilization, and costs of care. Jama. 2014; 311: 815-825. [CrossRef]
- Werner RM, Duggan M, Duey K, Zhu J, Stuart EA. The patient-centered medical home: an evaluation of a single private payer demonstration in New Jersey. Med Care. 2013; 51: 487-493. [CrossRef]
- Robert A. Petzel. VHA patient aligned care team (PACT) handbook. Washington, D.C: 2014. Available from: https://www.va.gov/VHAPUBLICATIONS/ViewPublication.asp?pub_ID=2977.
- Rosland AM, Nelson K, Sun H, Dolan ED, Maynard C, Bryson C, et al. The patient-centered medical home in the Veterans Health Administration. Am J Manag Care. 2013; 19: e263-272.
- Intrator O, Kelley K, Mor V. Veterans Health Administration geriatrics and expended care home and community-based programs. Innov Aging 2017; 1: 1328-1328. [CrossRef]
- Carolyn M. Clancy. Geriatric patient-aligned care team (GeriPACT). Washington, D.C: 2015. Available from: https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=3115.
- Sullivan JL, Eisenstein R, Price T, Solimeo S, Shay K. Implementation of the Geriatric Patient-Aligned Care Team Model in the Veterans Health Administration (VA). J Am Board Fam Med. 2018; 31: 456-465. [CrossRef]
- Gerontologic Society of America and the Hartford Foundation Change Agent Network: Patient Centered Medical Homes and the Care of the Older Adult. Dorr D, Schreiber R, Co- Chairs. Available from: https://changeagents365.org/resources/patient-centered-medical-home-network/Roadmap_PCMH_Change%20AGEnts.pdf (Accessed 8/9/2018).
- Sullivan JL, Adjognon OL, Engle RL, Shin MH, Afable MK, Rudin W, et al. Identifying and overcoming implementation challenges: Experience of 59 noninstitutional long-term services and support pilot programs in the Veterans Health Administration. Health Care Manage Rev. 2018; 43: 193. [CrossRef]
- Department of Veterans Affairs Transformational Funding Program for the 21st Century (T- 21). Available from: https://www.va.gov/LMR/docs/MOU_NFFE_T21_Healthcare_Transformation_Initiatives_6-9-2010.pdf (Accessed 8/9/2018).
- Bodenheimer T, Laing BY. The teamlet model of primary care. Ann Fam Med. 2007; 5: 457-461. [CrossRef]
- The Agency for Healthcare Research and Quality (AHRQ) -2014 estimates average cost hospital stay (4.5 days) 10,885, with per-diem 2,366. Available from: http://www.ahrq.gov/research/findings/factsheets/index.html/ (Accessed 8/9/2018).
- Palliative Care Research Cooperative Group. Average cost per medication per day $4. JAMA Intern Med. 2015; 175: 691-700.
- Dreyer T. Care transitions: best practices and evidence-based programs. Center for Healthcare Research & Transformation. Available from: https://www.chrt.org/publication/care-transitions-best-practices-evidence-based-programs/ (Accessed 8/9/2018).
- Hitch B, Parlier AB, Reed L, Galvin SL, Fagan EB, Wilson CG. Evaluation of a team-based, transition-of-care management service on 30-day readmission rates. NCMJ. 2016; 77: 87-92. [CrossRef]
- Jackson C, Shahsahebi M, Wedlake T, DuBard CA. Timeliness of outpatient follow-up: an evidence-based approach for planning after hospital discharge. Ann Fam Med. 2015; 13: 115-122. [CrossRef]
- Jackson CT, Trygstad TK, DeWalt DA, DuBard CA. Transitional care cut hospital readmissions for North Carolina Medicaid patients with complex chronic conditions. Health Affair. 2013; 32: 1407-1415. [CrossRef]
- Mansukhani RP, Bridgeman MB, Candelario D, Eckert LJ. Exploring transitional care: evidence-based strategies for improving provider communication and reducing readmissions. Pharmacy and Therapeutics. 2015; 40: 690.
- Rennke S, Ranji SR. Transitional care strategies from hospital to home: a review for the neurohospitalist. Neurohospitalist. 2015; 5: 35-42. [CrossRef]
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing Implement Sci. Implement Sci. 2009; 4: 50. [CrossRef]
- AAMC. Physician supply and demand through 2025: Key findings. Available from: https://www.aamc.org/download/450420/data/physiciansupplyanddemandthrough2025.pdf (Accessed 8/9/2018).
- Health Resources and Services Administration. Projecting the supply and demand for primary care practitioners through 2020. 2013. Available from: https://bhw.hrsa.gov/sites/default/files/bhw/nchwa/primarycarebrief.pdf
- HRSA. National and Regional Projections of Supply and Demand for Geriatricians: 2013- 2025. Available from: https://bhw.hrsa.gov/sites/default/files/bhw/health-workforce-analysis/research/projections/GeriatricsReport51817.pdf (Accessed 8/9/2018).
