

Missing Voices and Aging in Prison: Religiosity’s Influence on Positive Aging through Forgiveness
G. Kevin Randall 1, * ![]() , Alex J. Bishop 2
, Alex J. Bishop 2 ![]()
- Family & Consumer Sciences Department | College of Health Sciences, Sam Houston State University, Box 2177, Huntsville, USA
- Human Development and Family Studies, Stillwater, USA
* Correspondence: G. Kevin Randall ![]()
Academic Editor: Lisa A. Hollis-Sawyer
Special Issue: Got Aging? Examining Later-life Development from a Positive Aging Perspective
Received: August 24, 2018 | Accepted: November 5, 2018 | Published: November 7, 2018
OBM Geriatrics 2018, Volume 2, Issue 4 doi:10.21926/obm.geriatr.1804018
Recommended citation: Randall GK, Bishop AJ. Missing Voices and Aging in Prison: Religiosity’s Influence on Positive Aging through Forgiveness. OBM Geriatrics 2018;2(4):018; doi:10.21926/obm.geriatr.1804018.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
Background: This study investigated the influence of positive psychological predictors, religiosity and forgiveness, on subjective and objective successful aging outcomes among incarcerated males. Methods: Male prison inmates (N=261), aged 45 to 82 and incarcerated in eight state-managed correctional facilities, were sampled from the prison census database (Oklahoma Department of Corrections or DOC). Exclusion criteria, per the Oklahoma DOC, were those housed in medical or psychiatric units, currently in solitary confinement, or sentenced to death row. Results: The final mediation model fit the data well: MLR χ2 (df = 101, N = 256) = 7.40, p = .014, CFI = .98; RMSEA = .04 and SRMR = .03. With the exception of two direct effects, forgiveness mediated the relationship between religiosity and seven successful aging outcomes. Significant tests of total indirect effects through the three latent variable forgiveness mediators on each outcome were found; no specific indirect effects were significant. Analyses controlled for age, race, education, and crime type. Conclusions: Findings encourage continued investigations into the religiosity—forgiveness—health connection and specifically recommend forgiveness promoting interventions for all. For those incarcerated, interventions should include focus on forgiveness relative to earlier life trauma and abuse.
Keywords
Prisoner; mental health; physical health
1. Introduction
Recently, Rowe and Kahn [1] affirmed the need to expand upon their well-known model, rather than abandon it altogether. They noted that in a 2015 review of 67 papers critiquing their model [2] almost 70 percent of the papers suggested improving or expanding on the model because of its limited focus on disease, maintaining high cognitive and physical functioning, and engaging with life. Specifically, the review emphasized the social gerontology literature’s call for including the “missing voices” of older adults and other subjective constructs such as emotional well-being, social functioning, and religion. Further, Rowe and Kahn noted macrosocial changes influencing successful or positive aging. One such change, the aging of populations around the globe, creates many challenges, but is especially salient for the burgeoning U. S. prison population where the rate of increase in older prisoners is much higher relative to the overall population [3]. Thus, the present study, analyzing data provided by a convenience sample of incarcerated older males, expands concepts of positive aging in prison by positing and testing a model specifying the mediating role of forgiveness in the link between religiosity and seven outcomes associated with positive aging. The study’s findings provide potential implications for improving clinical applications of therapeutic forgiveness interventions used with older forensic populations who age-in-place, especially incarcerated males.
1.1 Expanding the Positive Aging Model: Religiosity—Forgiveness—Health
Almost thirty years have passed since Rowe and Kahn introduced the successful aging model; its useful generativity is illustrated in Martinson and Berridge’s [2] review of the social gerontology literature. They found 453 articles with successful aging in the title or text. Next, the authors imposed the need for an article to include a critique of successful aging ─ 67 articles comprised the final sample ─ and they applied qualitative methodology to conduct a configurative review. Forty-six articles proposed additional criteria for successful aging and recommended including older adults’ perspectives on more subjective measures. The present study built upon the classic objective outcomes of successful aging by including more subjective measures, or employing one of the review’s categories, “missing voices.” Further, the current study incorporated Pruchno and colleagues’ [4] work. They provided evidence that positive aging included objective and subjective indicators. This study investigated positive aging among older inmates (see Figure 1) and focused on the well-documented religion—forgiveness— health model, positing religiosity, mediated through measures of forgiveness, as significantly associated with subjective and objective positive aging outcomes. Our model’s subjective outcomes included valuation of life, self-perceived stress, depressive symptoms, and self-perceived health; the objective outcomes included a count of health conditions and physical activities of daily living. Further, as a research question, our model specified three types of forgiveness as mediators between religiosity and the successful aging outcomes. Theoretical and empirical rationale for the study’s model follows.
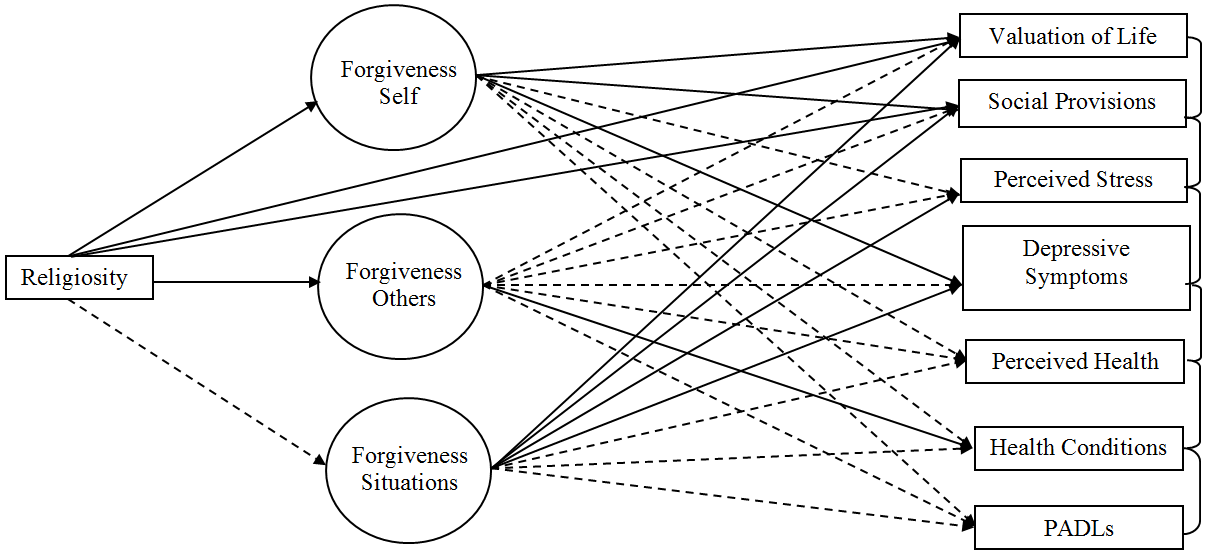
Figure 1 Final results of mediation model testing. Model Fit: Satorra-Bentler X2 (N=256; df =101) = 134.75; p = .014; CFI=.98; RMSEA=.04; SRMR=.03 (using FIML). Solid paths indicate p ≤ .05; dotted paths are p ≥ .051, two-tailed tests. Analyses controlled for age, race, education, and crime type; three mediator residuals were correlated as were residuals of the seven outcome measures.
Reviews regarding religion—health [5,6,7,8] are congruent with the review of Martinson and Berridge [2]. Though the associations can be complex, based upon the variety of measures and populations included in a study, the consensus in the literature is that religiosity/spirituality is positively associated with mental, behavioral, and physical health, in addition to reduced mortality. George and colleagues [8] noted that about one third of over 3,000 published quantitative reports examined the link between religion—health in samples of older adults, emphasizing the importance of these constructs when investigating older adults’ health outcomes and other aspects of positive aging. Furthermore, future research possibilities, in a number of published studies, call for investigations of the possible mechanisms linking religion—health outcomes [7,8,9,10]. Koenig [6] configured and described a theoretical model of causal pathways linking religion—health based on a comprehensive review of approximately 3300 quantitative articles. Religion, viewed as a coping mechanism, provided a pathway to mitigating negative emotional responses and associated negative or poor mental health assessments. For example, religion provides opportunity to reframe negative events and forgive self, others, and even situations; thus, religion or religiosity has been empirically shown to improve mental health. By extension, then, the influence of poor mental health is known to associate with poor physical health resulting in the hypothesis that religiosity would likely influence both mental and physical health outcomes through various mechanisms.
Therefore, the present study’s hypothesized model links religiosity to subjective and objective mental and physical health, positive aging criteria, through one of the links specified by Koenig’s model [6], namely dispositional forgiveness. Lavelock and colleagues [9] reviewed 95 studies on forgiveness and physical health. They then developed a conceptual model linking positive religious coping to better mental and physical health outcomes through forgiveness, in addition to other mediating mechanisms between forgiveness and health outcomes. Though models from these reviews included complex moderating and mediating pathways, they informed our hypothesized mediation model (Figure 1), allowing us to address some of the future recommendations for research agendas regarding these pathways of positive aging. Our model allowed a test of pathways suggested by the works referred to above, particularly the mediating role of forgiveness as postulated by Koenig [6] on mental and physical health outcomes.
Before turning to the present study’s mediator, forgiveness and the employed three subscales, we address the distinction between religiosity and spirituality, and why we use a well-known assessment for religiosity [11]. The question of differentiating religiosity from spirituality is addressed in most reviews and Koenig provided a succinct explanation drawn from the research base [6]. Religiosity and its activities lend themselves to measures of organizational association (e.g., religious affiliation) and activity (e.g., frequency of attendance) in addition to assessments of individual private practice and beliefs (e.g., prayer, reading, and salience of one’s beliefs). Measures of spirituality tend to have inherent challenges; they often include measures highly associated with aspects of positive psychological states resulting in the confounding of a predictor with its outcomes. For this study, we followed distinctions noted by Krause [12; pp. 9-10] and used a well-validated index of religiosity [11], assessing both organizational and individual activities.
Numerous studies have defined the concept of forgiveness [13,14,15]. Employing the Heartland Forgiveness Scale or HFS [13], we use an assessment of dispositional forgiveness. Further, HFS assesses, in addition to forgiving others, other aspects of forgiveness such as forgiving one’s self, and even forgiving uncontrollable life experiences such as illness, natural disaster, or other adverse situations. Forgiveness has been linked positively with mental and physical health outcomes [10,16,17,18], and with other variables related to positive aging, health outcomes (e.g., higher levels of agreeableness, low trait anger). Self-report measures of forgiving oneself or others often associate with various measures of positive physical health (e.g., lover levels of resting blood pressure, smoking, and alcohol use). In addition, using the HFS allowed us to extend previous work focusing on religiosity and forgiveness among incarcerated males [19] by specifying three latent variable mediators of forgiveness to explore whether or not differential or specific forgiveness pathways to successful aging outcomes exist. Thus, the present study’s model links religiosity through the three types of forgiveness to two types of positive aging outcomes, subjective and objective. Subjective positive aging outcomes included (a) an assessment of the overall meaning and value of one’s life at a point in time (i.e., valuation of life); (b) mental health (i.e., depressive symptoms and perceived stress); (c) social relationships and support (i.e., social provisions); and (d) physical health (i.e., perceived health). Objective positive aging outcomes included an assessment of (a) a lower number of reported health conditions and (b) physical activities of daily living or PADLs.
1.2 Positive Aging for Incarcerated Males
In addition to investigating the religion—forgiveness—health linkages, including at least two of the previously mentioned “missing voices” of positively aging older adults, namely religion and forgiveness, the present study gives voice to another audience regarding successful aging, older incarcerated males. Prisoner health care advocates and policy makers note with concern (a) the ever-increasing rate of older inmates and (b) that factors prior to and during imprisonment often result in prisoners’ physiological ages averaging 10 to 15 years more than their chronological ages [20,21]. Williams and colleagues [22] provided three substantive arguments for focusing on the well-being of older prisoners and the resultant need to set policy priorities: (1) the ever increasing growth in numbers and age of older prisoners and consequently, their escalating health care costs; (2) prisoner’s constitutional rights to access healthcare; and (3) since many prisoners are eventually released to the community, early identification and care for age-related physical and mental health challenges during imprisonment might improve their ability to function independently after release, resulting in decreased recidivism. For example, by law, prisoners receive annual examinations and necessary health care; in addition, our sample, by Oklahoma Department of Corrections advisement, excluded individuals at the extremes of the distribution of mental and physical health. As these individuals age, they seek many assets associated with positive aging such as good health, positive mental appraisals, and the encouragement and support of others. Since the theoretical and empirical work informing our hypothesized model is derived almost exclusively from non-incarcerated individuals, we investigate how well the model holds with our sample.
Thus, informed by the theoretical and empirical work reviewed, we conceptualized a mediational model linking religiosity to subjective and objective positive aging outcomes through three types of forgiveness. In addition, based upon the health supports provided incarcerated males, we believe that the model should hold in our sample. We predicted that (1) forgiveness would mediate the pathways from religiosity to the outcomes and that the indirect effects would be in expected directions; in other words, religiosity and forgiveness would relate positively with one another. In addition, we predicted the mediational path from religiosity through the facets of forgiveness would positively associate with outcomes of positive aging (e.g., valuation of life, social provisions, and physical activities of daily living) and negatively associate with the deficit aging outcomes (e.g., depressive symptoms, perceived stress, health conditions). As a research question, we specified three distinct mediators: forgiveness of self, forgiveness of others, and forgiveness of self in order to investigate possible differential relationships between religiosity and the successful aging outcomes.
2. Methods
2.1 Sample and Procedures
Participants were conveniently sampled from the prison census database maintained by the Oklahoma Department of Corrections (OK-DOC) Evaluation and Analysis Unit; participants were housed in eight state-managed, OK-DOC, correctional facilities. Following OK-DOC recommendations, exclusion criteria were used to protect the safety and well-being of inmates housed in medical or psychiatric units, currently serving time in solitary confinement, or sentenced to death row who might otherwise be vulnerable to threats of coercion. All exclusionary criteria were reviewed and approved via full board review by university IRB. Inmates were recruited through announcements circulated by prison administration (e.g., wardens, deputy wardens, unit managers), who also coordinated on-site data collection visits by trained members of the research team. The recruited sample included 262 older male inmates ages 45 to 82 (M =57.59, SD = 8.41). All participants read and signed a university (IRB) approved informed consent prior to participating in date collection or completing a written self-report survey. Those identified by prison administration as having reading difficulties as well as visual or auditory deficits were accommodated with a one-on-one private interview with a trained member of the research team. No monetary incentives were provided for participation.
The Oklahoma State University Institutional Review board approved this research on May 18, 2006 (OSU IRB HE0657) following Federal legislation 45CFR46.
2.2 Measures
Predictor Variable. Religiosity (REL) was assessed with two questions from the Duke Religion Index [11]. Participants were asked how often they attended church, synagogue, or other religious meetings and how often they spent time in private religious activities, such as prayer, meditation, or Bible study. Responses for attendance were assessed by a 6-point scale (1 = Never, 2 = Once a year or less, 3 = Few times a year, 4 = Few times a month, 5 = Once a week, and 6 = More than once a week). For private activities, responses were assessed by a 6-point scale (1 = Never, 2 = Once a year or less, 3 = Few times a month, 4 = Few times a week, 5 = Once a day, and 6 = More than once a day). The two questions correlated significantly (r = .71, p < .001); therefore, we summed the two, creating a composite variable (α = .83).
Three latent forgiveness mediators were derived from the Heartland Forgiveness Scale or HFS [13,14]. The HFS is an 18-item self-report measure of dispositional forgiveness comprised of three subscales. We used item parceling on each subscale to create three indicators for: forgiveness of self (FSelf; e.g., “Although I feel badly at first when I mess up, over time I can give myself some slack”); forgiveness of others (FOthers; e.g., “With time I am understanding of others for the mistakes they’ve done”); and forgiveness of situations (FSit; e.g., “Eventually, I let go of negative thoughts and bad circumstances that are beyond anyone’s control”). Items were scored on a 7-point scale (1 = Almost always false of me to 7 = Almost always true of me). Higher scores indicated higher levels of forgiveness. Internal consistency for each of the three subscales was acceptable (self, α = .67; other, α = .79; and situations, α = .62). However, to model these mediators of interest, accounting for measurement error, three indicators for each latent assessment of forgiveness were created via item parceling. Regarding item parceling to create indicators for the three forgiveness latent variables, Little and colleagues [23] proposed that the purpose of the study at hand should determine whether or not parceling is appropriate. Similarly, Coffman and MacCallum [24] recommended researchers primarily interested in investigating the relationships between constructs, or mediational pathways, employ the use of latent variables with parcels as indicators, modeling measurement error rather than conduct path analysis with its assumption of constructs measured without error. Thus, the present study focused on the indirect effects of religiosity on successful aging outcomes through latent mediators assessing three types of forgiveness.
Outcome Variables. The thirteen positive items (α = .88) from Lawton’s Valuation of Life scale [25] or VOL were used. Assessed on 5-point scales (1 = strongly disagree to 5 = strongly agree), higher scores reflected greater life value. The developers constructed the scale with items from five core constructs: (1) futurity (i.e., the future is worth anticipating); (2) hope (i.e., what happens now and in the future will be positive); (3) self-efficacy (i.e., the individual will demonstrate competence in the future); (4) persistence (i.e., efforts to problem solve are worthwhile and will likely lead to success); and (5) purpose (i.e., agreement regarding goals that guide the participant’s life choices).
Social provisions were evaluated with the 24-item Social Provisions Scale or SP [26]. SP measures the degree to which respondent’s social ties provide guidance (e.g., There is a trustworthy person I could turn to for advice, if I were having problems), reassurance (e.g., I have relationships where my competence and skill are recognized), social integration (e.g., There are people who enjoy the same social activities I do), attachment (e.g., I have close relationships that provide me with a sense of emotional security and well-being), nurturance (e.g., I feel personally responsible for the well-being of another person), and reliable alliance (e.g., There are people I can depend on to help me, if I really need it). Items were scaled from 1 (strongly disagree) to 4 (strongly agree) and summed to create a composite variable, SP; α = .91.
The 14-item Perceived Stress Scale or PS [27] assessed the degree to which past month life situations were appraised as stressful by the participant. Sample items included, “In the last month, how often have you dealt successfully with irritating life hassles? ” and “In the last month, how often have you felt nervous or stressed? ” Items were scored 1 = Never, 2 = Almost never, 3 = Sometimes, 4 = Fairly often, and 5 = Very often, and then summed to create the variable with higher scores reflecting higher feelings of stress; α = .82.
Depressive symptoms were assessed using the 10-item short form Geriatric Depression Scale or GDS [28]; α = .85. Sample questions included “Do you often feel downhearted and blue? ” and “Do you feel pretty worthless the way you are now? ” Responses were scored 0 (No) or 1 (Yes) and the items summed creating a global depression score ranging from 0 to 10, with higher scores representing higher levels of depressive symptoms.
Four items from the Subjective Health Perceptions Scale from the Older Americans Resources and Services or OARS [29] assessed perceived health. Examples of questions include, “How would you rate your overall health at the present time? ” (1= poor and 4 = excellent); and “How much do health troubles stand in the way of you doing the things you want to do? ” (1 = not at all and 4 = a great deal). Higher scores indicated greater perceived health; α = .81.
Health conditions or HC were assessed with a 14-item self-report checklist. Health conditions related to heart health (e.g., heart attack, heart murmur), respiratory problems (e.g. asthma, emphysema), organ functioning (e.g., liver disease) and other chronic conditions (e.g., high blood pressure, high cholesterol, diabetes, hepatitis). Participants were asked to check all health conditions they had experienced within the last year. Items were summed to create a composite measure of health conditions ranging from 0 (presence of no health conditions) to 14 (presence of all health conditions).
Six items from the OARS [29] assessed physical activities of daily living (PADLS). Sample questions included, “Can you eat? ” and “Can you get in and out of bed? ” Responses were scored 1 = Completely unable, 2 = With some help, and 3 = Without help and the items summed so that higher scores represented higher levels of functional ability; α = .77.
Controls. Demographic control variables included age, race, education, and crime type. We recoded race so that 0 (White) and 1 (non-White). Education was treated as a continuous variable with scores from 1 (completed grade school or less) to 9 (earned a doctoral degree). Crime type, a dichotomous measure, was coded 0 = non-violent (e.g., fraud, burglary, vandalism) and 1 = violent (e.g., manslaughter, rape, murder).
2.3 Data Analytic Technique
Descriptive statistics and bivariate correlations were computed using SPSS 22.0. To test the mediation model we employed Mplus 7.4 with full information maximum likelihood or FIML [30] to account for missing data. We used the MLM estimator that calculates maximum likelihood parameter estimates (and 95% confidence intervals) with standard errors and a mean-adjusted chi-square test statistic that are robust to non-normality. To arrive at the best fitting model, we employed nested modeling procedures [31]. All endogenous variables were controlled for age, race, education, and crime type. In addition to the chi-square goodness of fit test, we report the Comparative Fit Index (CFI); the root mean squared error of approximation (RMSEA); and the standardized root mean squared residual (SRMR). Values close to or greater than .95 for CFI, and less than .08 for SRMR and .06 for RMSEA, suggest a relatively good model fit [32]. Further, we report 95% confidence intervals for regression (i.e., gamma and beta coefficients) parameters and indirect effects.
3. Results
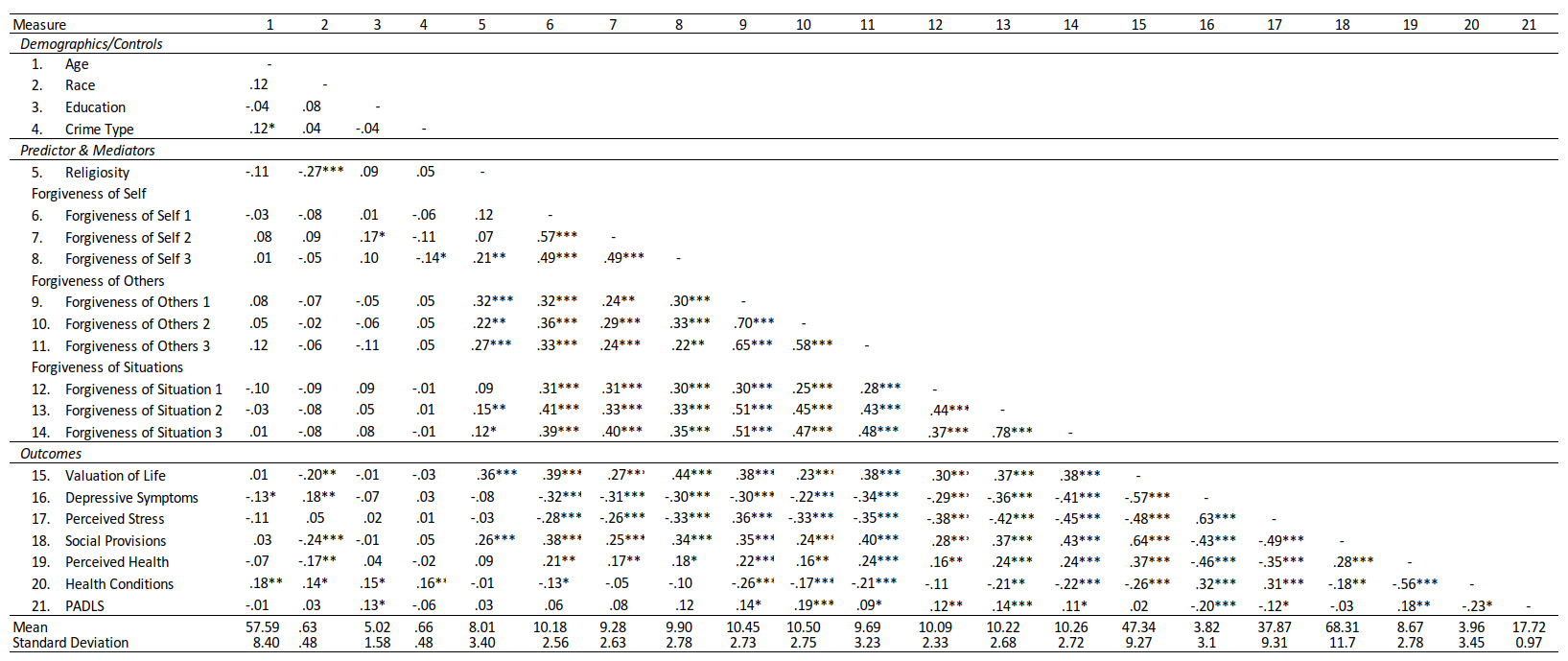
First, sample characteristics (e.g., race, education, crime type, and sentence length; see Table 1) and descriptive statistics (e.g., means, standard deviations, and bivariate correlations; Table 2) were computed for all 21 study variables. The bivariate correlations among the study variables revealed expected and significant associations. For example, REL was associated with indicators of FSelf, FOthers, and FSit, in addition to outcomes VOL and SP. In addition, all of the forgiveness indicators were significantly and positively correlated with the healthy aging outcomes with one exception: the indicators of FSelf were not significantly associated with PADLS.
Second, we tested the measurement model and then the hypothesized model with religiosity predicting the seven outcomes through the specified latent variable forgiveness mediators, following the recommendations of Coffman and MacCallum [24] as mentioned above. The latent variable measurement model consisting of the three mediators, FSelf, FOthers, and FSit, fit the data well: MLR χ2 (df = 24, N = 255) = 28.02, p = .26, CFI = .99; RMSEA = .03 and SRMR = .03. All factor loadings were substantive and significant p < .001 (see Table 3). Next, we tested the hypothesized complete mediation model (no direct paths specified) controlling endogenous variables (mediators and outcomes) for age, race, education, and crime type. Model fit and modification indices led us to respecify the model and include two direct paths from REL to VOL and SP (Figure 1). This final model fit the data well: MLR χ2 (df = 101, N = 256) = 7.40, p = .014, CFI = .98; RMSEA = .04 and SRMR = .03. In Figure 1, solid lines represent significant regression paths; dotted represent non-significant paths.
Table 1 Sample Characteristics

Table 2 Means, Standard Deviations, and Bivariate Correlations for Model Variables
For the sake of presentation simplicity, we provide two tables of parameter estimates for this final model’s estimates (i.e., together, Table 4 and Table 5 provide the regression parameter estimates, significance levels, and 95% CIs for the paths in Figure 1). Though a number of parameter estimates are significant based on directional hypotheses and one-tailed tests, due to the number of parameters estimated and the complexity of the model, we only report significant results at the p ≤ .05 (two-tailed test) and those that do not have zero in the 95% CI. The estimates of the direct effects (and 95% confidence intervals) of REL on FSelf, Fothers, Fsit, VOL, and SP are provided in Table 4. With the exception of FSit (γ=.13, p = .064, 95% CI [-.007, .256]), the parameter estimates regressing the other latent mediating variables and the two outcomes, VOL and SP, directly on REL were significant and in the hypothesized direction. Similarly, for the sake of presentation simplicity, Table 5 provides the parameter estimates and 95% CIs for the regression of the seven outcomes on the three latent mediators in the final full mediation model. As predicted, each outcome was significantly associated with one of the forgiveness mediators; three outcomes were significantly associated with FSelf (VOL, GDS, and SP), one with FOthers (HC), and four with FSit (VOL, GDS, PS, SP). Of note and contrary to our predictions: (1) PADLS was not significantly associated with any of the three forgiveness mediators and (2) only HC significantly associated with FOthers (β = -.17, p = .05, 95% CI [-.35, .001]).
Last, tests of indirect effects are reported in Table 6. Addressing our research questions relative to the three different types of forgiveness, Table 6 shows there were no specific indirect effects from REL through one type of forgiveness mediator to an outcome. However, significant total indirect effects (the sum of the effects through the three mediators) were found for each of the seven outcomes.
Table 3 Latent Variable Measurement Model Results
Table 4 Model Estimates, direct paths [and 95% Confidence Intervals] of Forgiveness Types and Valuation of Life† and Social Provisions† on Religiosity (Standardized Coefficients)
Table 5 Model Estimates [95% Confidence Intervals] and R2 of Types of Forgiveness On Outcomes (Standardized Coefficients) controlling for Religiosity
Table 6 Total (across the three mediators) Indirect Effects (two-tailed tests; standardized)
4. Discussion
Based on suggestions to (a) expand the model of positive aging by including subjective and often missing voices of constructs that matter to the older adults, but are often “ignored” [1]; (b) consider the health and well-being of the increasing population of older incarcerated prisoners [3]; and (c) to respond to the volume of work related to religion—forgiveness— health [8,9,33]; we tested a mediational model linking religiosity to subjective and objective outcomes often associated with salubrious and positive aging through three aspects of forgiveness. Results supported the hypothesized model but indicated that forgiveness as a whole mediated the link between religiosity and positive aging outcomes, and not specific constructs of forgiveness: self, others, or situations. We discuss the significance of the overall findings and, in particular, the total indirect effects through forgiveness. After noting the study’s limitations, we focus on the implications of our findings for overall prisoner well-being, therapeutic options relative to rehabilitation, and lower recidivism for those released.
Overall, this study adds to the literature assessing aspects of positive or healthy aging, particularly the “missing” and often subjective voices found in the religion—forgiveness—health linkage [2]. Table 5 demonstrates that in the full model, when the outcomes are regressed through the latent mediators and onto religiosity, a large amount of variance is explained (controlling for age, race, education, and crime type). For those outcomes considered subjective or based on the individual’s perceptions, approximately 30-40 percent of the variance was explained when including religiosity and forgiveness. For valuation of life and social provisions, both direct effects from religiosity and indirect effects through forgiveness, were found. Further, we also note that our research question, relative to the differing types of forgiveness, resulted in the total or the summed indirect effects through the three types of forgiveness on the outcomes, but not through specific indirect effects from religiosity to an outcome. This finding could be based on limited power to detect the effects if present (i.e., three of the indirect effects reached one-tailed significance) or simply a confound of the specific measure employed. Knowing whether or not prisoners in our sample believed they had received forgiveness, were seeking forgiveness, and currently felt “unforgiven,” might influence our findings (e.g., a majority of the study’s sample were violent offenders) relative to the indirect effects. Further investigation surrounding the status of forgiveness among older prisoners is warranted. However, such assessment was beyond the scope of the present study.
Thus, our results, based on data provided by a unique sample—older incarcerated males—supported and expanded upon recent reviews [2,7] of positive aging, demonstrating clearly the important influence of the associations among the study’s variables. At the same time, it is important to note that the literature informing our hypothesized model was primarily based on non-prison samples and thus, our findings are comparable and consistent with others to date. Importantly then, what implications do our findings have for those behind bars? Three reviews, (1) a meta-analysis by Wade et al. [34]; (2) a review by Elliott [35] on the efficacy of psychotherapeutic interventions to promote forgiveness and physical health; and (3) a review by Leach et al. [36] on recidivism and its association with traumatic grief inform our discussion -- in addition to recent work by Maschi et al. [37] -- inform our discussion of the study’s implications and recommendations for future research.
Taken together with the extant literature, our study underscores the important role played by forgiveness in association with positive aging, and it follows that interventions designed to promote forgiveness should prove helpful. Wade and colleagues [34] reviewed 54 reports on forgiveness interventions and concluded that indeed forgiveness is a viable, evidence-based treatment technique. Yet, for those incarcerated, it may depend. For example, Elliott [35] noted that future efforts on forgiveness-promoting interventions need to include a focus on the participants’ unique personal and social health. In other words, the life histories of individuals participating in such efforts need to be considered ahead of time: some aspects of forgiving and feeling forgiven may come easier than others and especially for some individuals. Work by Maschi and colleagues [37] affirms this point; they found that prisoners tend to share lifelong experiences of multiple traumas, stress, grief, separation and loss, placing them at risk for achieving later-life positive aging outcomes. Further, Leach et al. [36] found that childhood trauma, abuse, and bereavement rates were much higher in the prison population, leading to unresolved trauma and higher recidivism rates. Their figure (p. 116) compared the outcomes of resolved and unresolved traumatic grief in prisoners: accepting the loss/losses and moving on versus recidivism.
The study’s limitations include threats to internal and external validity. Regarding internal validity the data analyzed is cross-sectional and therefore, the modeling results, though based on theoretical and empirical research, cannot address causal direction or bi-directionality. In addition, the specified mediating effects may not have had time to unfold and influence the purported outcomes, leading to the null results in our findings; future research would want to include longitudinal data in order to detect such indirect effects. We employed measures considered appropriate for health outcomes (e.g., dispositional forgiveness) but the religion—forgiveness—health empirical literature is expansive [7,15,33]. Future research may wish to consider a prospective longitudinal design and a systematic review of measures used in various contexts. Further, a mixed-methods or qualitative focus including participants’ reflection relative to the role of religiosity and forgiveness on coping with incarceration would be of value for future investigations. Last, though this study did not have a control group (i.e., we argued that the existing results derived from non-prisoner samples acted as a proxy control) and though the OK-DOC explained the difficulty with building a released-prisoner sample, researchers embracing the challenges of finding and assessing formerly incarcerated individuals would help address how the context of prison moderates the links related to positive aging outcomes for those no longer incarcerated. In addition, a longitudinal study focused on aging-in-prison would do similar for those living out their lives behind bars and inform prison health-care in particular.
Therefore, despite limitations, the study’s findings encourage continued investigations into the religiosity—forgiveness—health connection and specifically recommend forgiveness promoting interventions for positive aging outcomes. . However, for those incarcerated, interventions should include focus on forgiveness relative to earlier life trauma and abuse. Engaging in a forgiveness intervention that includes acknowledgement and resolution of traumatic grief may lead to greater outcomes of prisoner well-being, rehabilitation and for those released, lower levels of recidivism.
Author Contributions
Dr. Randall contributed to the analysis, writing and revisions of the manuscript. Dr. Bishop contributed to the data acquisition, design, writing and revisions of the manuscript.
Funding
State the organization(s) or foundation(s) that funded this research.
Competing Interests
The authors have declared that no competing interests exist.
References
- Rowe JW, Kahn, RL. Successful aging 2.0: conceptual expansions for the 21st Century. J Gerontol B: Psychol Sci and Soc Sci. 2015; 70: 593-596. [CrossRef]
- Martinson M, Berridge, C. Successful aging and its discontents: a systematic review of the social gerontology literature. Gerontologist. 2015; 55: 58-69. [CrossRef]
- Porter LC, Bushway SD, Tsao H, Smith HL. How the U.S. prison boom has changed the age distribution of the prison population. Criminology. 2016; 54: 30-55. [CrossRef]
- Pruchno RA, Wilson-Genderson M, Rose M, Cartwright F. Successful aging: early influences and contemporary characteristics. Gerontologist. 2010; 50: 821-833. [CrossRef]
- Chida Y, Steptoe A, Powell LH. Religiosity/spirituality and mortality: a systematic quantitative review. Psychother Psyhosom. 2009; 78: 81-90. [CrossRef]
- Koenig HG. Religion, spirituality, and health: the research and clinical implications. ISRN Psychiatry. 2012; doi:10.5402/2012/278730. [CrossRef]
- Koenig HG. Religion, spirituality, and health: a review and update. Adv Mind Body Med. 2015; 29: 19-26.
- George LK, Kinghorn WA, Koenig HG, Gammon P, Blazer DG. Why gerontologists should care about empirical research on religion and health: transdisciplinary perspectives. Gerontologist. 2013; 53: 898-906. [CrossRef]
- Lavelock CR, Snipes DJ, Griffin BJ, Worthington EL Jr, Davis DE, Hook JN, et al. Forgiveness and health: scientific evidence and theories relating forgiveness to better health. Dordrecht: Springer Science+Business Media; 2015. (p. 29-42).
- Lawler-Row KA. Forgiveness as a mediator of the religiosity—health relationship. Psycholog Relig Spiritual. 2010; 2: 1-16. [CrossRef]
- Koenig HG, Meador K, Parkerson G. Religion index for psychiatric research: a 5-item measure for use in health outcome studies. Am J Psychiatry. 1997; 154: 885-886. [CrossRef]
- Krause N. Aging in the church: how social relationships affect health. West Conshohocken: Templeton Foundation Press; 2008.
- Thompson LY, Snyder CR. Positive psychological assessment: a handbook of models and measures. Washington: American Psychological Association; 2003. (p. 301-312). [CrossRef]
- Thompson LY, Snyder CR, Hoffman L, Michael S, Rasmussen HN, Billings LS, et al. Dispositional forgiveness of self, others, and situations. J Pers. 2005; 73: 313-359. [CrossRef]
- Tucker JR, Bitman RL, Wade NG, & Cornish MA. Forgiveness and health: scientific evidence and theories relating forgiveness to better health. Dordrecht: Springer Science+Business Media; 2015. (p. 13-28).
- Berry JW, Worthington EL. Forgiveness, relationship quality, stress while imagining relationship events, and physical and mental health. J Couns Psychol. 2001; 48: 447-455. [CrossRef]
- Lawler KA, Younger JW, Piferi RL, Jobe RL, Edmondson KA, Jones WH. The unique effects of forgiveness on health: An exploration of pathways. J Behav Med. 2005; 28: 157-167. [CrossRef]
- Wade NG, Worthington EL. Overcoming interpersonal offenses: is forgiveness the only way to deal with unforgiveness?. J Couns Dev. 2003; 81: 343-353. [CrossRef]
- Randall GK, Bishop AJ. Direct and indirect effects of religiosity on valuation of life through forgiveness and social provisions among older incarcerated males. Gerontologist. 2013; 53: 51-59. [CrossRef]
- Aday RH. Aging prisoners: crisis in American corrections. Westport: Praeger; 2003.
- Loeb SJ, AbuDagga A. Health-related research on older inmates: an integrative review. Res Nurs Health. 2006; 29: 556-565. [CrossRef]
- Williams BA, Stern MF, Mellow J, Safer M, Greifinger RB. Aging in correctional custody: setting a policy agenda for older prisoner health care. Am J Public Health. 2012; 102: 1475-1481. [CrossRef]
- Little TD, Cunningham WA, Shahar G, Widaman KF. To parcel or not to parcel: exploring the question, weighing the merits. Struct Equ Modeling. 2002; 9: 151-173. [CrossRef]
- Coffman DL, MacCallum RC. Using parcels to convert path analysis models into latent variable models. Multivariate Behav Res. 2005; 40: 235-259. [CrossRef]
- Lawton MP, Moss M, Hoffman C, Kleban, MH, Ruckdeschel K, Winter L. Valuation of life: a concept and a scale. J Aging Health. 2001; 13: 3-31. [CrossRef]
- Cutrona CE, Russell D. Advances in personal relationships. Vol. 1. Greenwich: JAI Press; 1987. (p. 37-67).
- Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983; 24: 385-396. [CrossRef]
- Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986; 5: 165-173. [CrossRef]
- Fillenbaum GG. Multidimensional functional assessment of older adults: the Duke Older Americans Resources and Services procedures. Hillsdale: L. Erlbaum; 1988.
- Graham JW. Missing data analysis: making it work in the real world. Annu Rev Psychol. 2009; 60: 549-576. [CrossRef]
- Raykov T, Marcoulides GA. A first course in structural equation modeling. 2nd ed. Mahwah: Lawrence Erlbaum Associates, Publishers; 2006.
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999; 6: 1-55. [CrossRef]
- Witvliet CVO, Tongeran VDR, Luna LR. Forgiveness and health: scientific evidence and theories relating forgiveness to better health. Dordrecht: Springer Science+Business Media; 2015. (p. 13-28).
- Wade NG, Hoyt WT, Kidwell JEM, Worthington EL Jr. Efficacy of psychotherapeutic interventions to promote forgiveness: a meta-analysis. J Consult Clin Psychol. 2014; 82: 154-170. [CrossRef]
- Elliott BA. Forgiveness and health: scientific evidence and theories relating forgiveness to better health. Dordrecht: Springer Science+Business Media; 2015. (p. 271-285).
- Leach RM, Burgess T, Holmwood, C. Could recidivism in prisoners be linked to traumatic grief?. a review of the evidence. Int J Prison Health. 2009; 4: 104-119. [CrossRef]
- Maschi T, Viola D, Morgen K, Koskinen L. Trauma, stress, grief, loss, and separation among older adults in prison: the protective role of cooping resources on physical and mental well-being. J Crime Justice. 2015; 38: 113-136. [CrossRef]
