

Behavioral Symptoms of Dementia
Ladislav Volicer * ![]()
- School of Aging Studies, College of Arts and Sciences, University of South Florida, Tampa, FL, 33620, USA
* Correspondence: Ladislav Volicer ![]()
Special Issue: Behavioral Symptoms of Dementia
Received: November 04, 2018 | Accepted: November 05, 2018 | Published: November 08, 2018
OBM Geriatrics 2018, Volume 2, Issue 4 doi:10.21926/obm.geriatr.1804019
Recommended citation: Volicer L. Behavioral Symptoms of Dementia. OBM Geriatrics 2018; 2(4): 019; doi:10.21926/obm.geriatr.1804019.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
The number of people having some type of dementia is increasing worldwide, because people live longer, and increased age is the most important risk factor for development of these diseases. Currently, we do not have any effective medications for Alzheimer’s disease and other progressive degenerative dementias. This that does not mean that we cannot do anything to help these people, it is actually possible to help them maintain quality of life despite the progressive deterioration of their cognitive functions.
Quality of life for people with dementia requires addressing three main areas: psychological needs, medical issues, and behavioral symptoms (Figure 1). Psychological needs are addressed by availability of meaningful activities, which provide a reason for people with dementia to get up every morning, increase their self-esteem, and prevent boredom. People with moderate dementia require continuous activity programming for all their waking hours [1] and people with advance and terminal dementias require modified activities of daily living in a group setting, so they are not isolated and are in presence of others [2]. Medical issues in people with advanced and terminal dementia are best addressed by a palliative care approach, which eliminates some aggressive medical interventions that cause more burden than benefits, e.g., cardiopulmonary resuscitation, transfer to acute care setting, tube feeding and use of antibiotics for treatment of generalized infections [3,4].
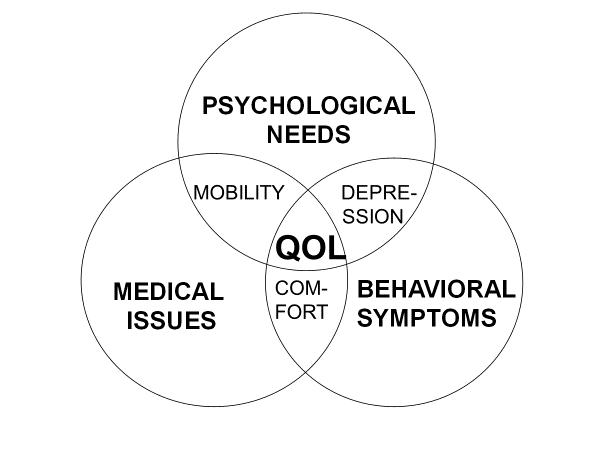
Figure 1 Components of quality of life in people with dementia
Both of these areas, of course interact with the third main area, behavioral symptoms. Some behavioral symptoms, e.g., agitation, can be prevented by elimination of boredom while some behavioral symptoms may be elicited by medical interventions that evoke discomfort. Thus, it is important to eliminate treatable causes of abnormal behaviors, before they are ascribed to dementia. There are several risk factors for development of behavioral symptoms of dementia (Table 1). The most important risk factors for development of rejection of care, which may result in abusive behavior, are depression and poor communication between the person with dementia and his/her care provider.
Table 1 Risk factors for development of abnormal behaviors in dementia
|
Environmental |
Temperature, noise, physical barriers |
|
Physical |
Pain, infection, hunger, thirst |
|
Psychiatric conditions |
Depression, delusions, hallucinations |
|
Cognitive impairment |
Lack of understanding, boredom |
Almost half of the people with dementia develop symptom of depression [5]. One of the reasons for this is damage of serotoninergic brain areas present in Alzheimer’s disease [6] and possibly also in other dementia types. There is some controversy about effectiveness of antidepressants in decreasing behavioral symptoms of dementia. But lack of antidepressants effects on behavior in some studies could have been due to insufficient therapy. The analysis of DIADS study, which divided participants according to effectiveness of antidepressant therapy, clearly showed that when depression was decreased so were decreased behavioral symptoms [7]. The other reason might have been that antidepressants are often not effective alone but required augmentation with atypical antipsychotics [8].
Depression may actually cause abusive behavior even without presence of rejection of care [9]. In addition, results of a longitudinal study indicated that depression is also a factor in development of agitation. Symptoms of depression were more common in persons who were agitated, and agitation increased and decreased together with changes of symptoms of depression prevalence [10]. There are some activity programs that decrease both the agitation and symptoms of depression [11,12].
The lack of understanding of care providers’ intentions, and of need for the care activity, is the second most important risk factor for development care rejection (Figure 2). A longitudinal study showed that changes in lack of understanding predicted changes in rejection of care. Changes of behaviors directed towards others were related to changes in lack of understanding and depression. Mediation models suggested that only the relationship of lack of understanding with behaviors directed towards others was mediated by rejection of care [13]. Therefore, improvement in communication between residents and caregivers may prevent or ameliorate these behaviors directed towards others [14].

Figure 2 Factors related to resistiveness to care (1 = resist care 1-3 days/week, 2 = resist care 4-6 days/week, 3 = resist care daily), data from [9]
We hope that papers in this special issue will further elucidate causes of behavioral symptoms of dementia and suggest strategies for their management.
Author Contributions
This work was completed by the single author.
Competing Interests
The author has declared that no competing interests exist.
References
- Volicer L, Simard J, Pupa JH, Medrek R, Riordan ME. Effects of continuous activity programming on behavioral symptoms of dementia. J Am Med Dir Assoc. 2006; 7: 426-431. [CrossRef]
- Simard J. The end-of-life namaste program for people with dementia. 2nd ed. Baltimore, London, Sydney: Health Professions Press; 2013.
- Volicer L. Palliative care in dementia. Progress in Palliative Care. 2013; 21: 146-150. [CrossRef]
- van der Steen JT, Radbruch L, Hertogh CM, de Boer ME, Hughes JC, Larkin P, et al. White paper defining optimal palliative care in older people with dementia: a Delphi study and recommendations from the European Association for Palliative Care. Palliat Med. 2014; 28: 197-209. [CrossRef]
- Volicer L, Frijters DH, Van der Steen JT. Underdiagnosis and undertreatment of depression in nursing home residents. Eur Geriatr Med. 2011; 2: 332-337. [CrossRef]
- Yamamoto T, Hirano A. Nucleus raphe dorsalis in Alzheimer's disease: neurofibrillary tangles and loss of large neurons. Ann Neurol. 1985; 17: 573-577. [CrossRef]
- Lyketsos CG, DelCampo L, Steinberg M, Miles Q, Steele CD, Munro C, et al. Treating depression in Alzheimer disease - Efficacy and safety of sertraline therapy, and the benefits of depression reduction: The DIADS. Arch Gen Psychiatry. 2003; 60: 737-746. [CrossRef]
- Papakostas GI, Shelton RC, Smith J, Fava M. Augmentation of antidepressants with atypical antipsychotic medications for treatment-resistant major depressive disorder: a meta-analysis. J Clin Psychiatry. 2007; 68: 826-831. [CrossRef]
- Volicer L, Van der Steen JT, Frijters D. Modifiable factors related to abusive behaviors in nursing home residents with dementia. J Am Med Dir Assoc. 2009; 10: 617-622. [CrossRef]
- Volicer L, Frijters DH, Van der Steen JT. Relationship between symptoms of depression and agitation in nursing home residents with dementia. Int J Geriatr Psychiatry. 2012; 27: 749-754. [CrossRef]
- Soliman A, Hirst S. Using sensory activities to improve dementia care. Nursing Times. 2015; 111: 12-15.
- Joranson N, Pedersen I, Rockstad AM, Ihlebaek C. Effects on symptoms of agitation and depression in persons with dementia participating in robot-assisted activity: A cluster-randomized controlled trial. J Am Med Dir Assoc. 2015; 16 : 867-873. [CrossRef]
- Galindo-Garre F, Volicer L, Van der Steen JT. Factors related to rejection of care and behaviors directed towards others: a longitudinal study in nursing home residents with dementia. Dement Geriatr Cogn Dis Extra. 2015; 5: 123-134. [CrossRef]
- Sloane PD, Honn VJ, Dwyer SAR, Wieselquist J, Cain C, Meyers S. Bathing the Alzheimer's patient in long term care. Results and recommendations from three studies. Am J Alzheim Dis. 1995; 10: 3-11. [CrossRef]
