

Leveraging Mindfulness to Build Resilience and Professional Quality of Life in Human Service Professionals
Andrew Hanna 1,*![]() , Aileen M. Pidgeon 2
, Aileen M. Pidgeon 2![]()
- School of Health and Human Sciences, Southern Cross University, Coffs Harbour, NSW, Australia 2450
- Faculty of Society and Design, Bond University, QLD, Australia 4229
* Correspondence: Andrew Hanna![]()
Received: April 4, 2018 | Accepted: May 7, 2018 | Published: May 16, 2018
OBM Integrative and Complementary Medicine 2018, Volume 3, Issue 2 doi:10.21926/obm.icm.1802007
Academic Editor: Sok Cheon Pak
Special Issue: Health Benefits of Meditation
Recommended citation: Hanna A, Pidgeon A. Leveraging Mindfulness to Build Resilience and Professional Quality of Life in Human Service Professionals. OBM Integrative and Complementary Medicine 2018;3(2):007; doi:10.21926/obm.icm.1802007.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
Objective: Mindfulness-based interventions (MBIs) have shown promise in cultivating resilience and are widely accepted as efficacious in the treatment of a range of psychological disorders. This paper explores the feasibility of a mindful-awareness and resilience skills training (MARST) program to enhance mindfulness and resilience, as a means of increasing psychological well-being and alleviating burnout and compassion fatigue in human service professionals.
Method: In this randomised control trial, 46 human service professionals were randomly allocated to either a MARST group or to a no intervention, control group.
Results: Multivariate analysis of covariance (MANCOVA), with pre-test scores as the covariates, revealed that the MARST intervention resulted in significant improvements in mindfulness, resilience, compassion satisfaction, and psychological well-being, and significant reductions in burnout and compassion fatigue; at post-intervention. These results were maintained at one month follow-up, with the exception of compassion satisfaction which was non-significant. Mediation analysis using a bootstrap resampling method indicated that mindfulness fully mediated changes in resilience and psychological well-being, as a result of the MARST intervention. Self-reported reductions in burnout following the intervention were mediated by mindfulness and resilience, and decreased compassion fatigue was mediated by resilience.
Conclusions: The results of this study suggest that the MARST program may assist in developing resilience and reduce burnout and compassion fatigue in human service professionals. The study also provides evidence for the potential of mindfulness-based approaches to enhance resilience.
Keywords
Resilience; mindfulness; compassion fatigue; burnout; psychological well-being
Key Points
1. Human service professionals are at risk of compassion fatigue and burnout.
2. Strategies that cultivate resilience may ameliorate the development of these conditions.
3. Mindfulness-based interventions have been shown to build resilience.
4. MARST may assist in developing resilience and reduce burnout and compassion fatigue in human service professionals.
5. The observed change in resilience was mediated by mindfulness.
6. The change in compassion fatigue was mediated by resilience and mindfulness.
1. Introduction
Over the past two decades, research has demonstrated that prolonged exposure to the pain and suffering of others may have deleterious effects on psychological well-being and functioning [1,2]. Evidence also suggests that those who work with individuals with mental illness, addiction, social deprivation, and trauma may suffer similar and often debilitating consequences [3,4,5]. As an occupational group, human service professionals are concerned with the intervention and empowerment of clinical and otherwise vulnerable social populations. As a result, practitioners are routinely confronted with the psychological distress, emotional pain and traumatic recollections of the individuals with whom they work [6]. Indeed, researchers who have examined the occupational hazards of the human services have stressed that the process of caring itself, may come at significant personal and psychological costs [4,7].
The “cost of caring” was first described by Figley [8] who identified compassion fatigue (or secondary traumatic stress) as the potential consequence of bearing witness to the suffering of others. Defined as a state of tension and preoccupation with the traumatised client, compassion fatigue describes a syndrome which often parallels the symptoms of post-traumatic stress disorder (PTSD[4]). Human service professionals who experience compassion fatigue are also at an increased risk of developing psychological conditions, such as mood and anxiety disorders [9]; substance dependence [10]; eating disorders [11]; suicide [12]; and clinician burnout [4].
Burnout refers to a multifaceted work-related disorder which occurs when professionals have insufficient resources to handle excessive occupational demands [13]. Those affected describe feelings of being over-extended, fatigued, and depleted; attitudes of negativity and cynicism; and a reduced sense of accomplishment [14]. Burnout among human service professionals is also considered to contribute to a number of adverse organisational consequences including; increased staff turnover and absenteeism, unproductive work behaviours, and reduced job-satisfaction [15,16]. Therefore, practitioner-focused research has recognised the need to understand the factors which safeguard clinician mental health and explain why some professionals develop these conditions, while others do not.
This growing interest in resilience represents a shift from the traditional focus on psychopathology, to an emphasis on the protective factors which promote a healthy response to stress [17]. Although a universal definition does not exist, resilience is considered an individual’s capacity to overcome adversities that would otherwise be expected to have negative consequences [18]. The development of resilience may serve to ameliorate or buffer the impact of occupational stressors and protect clinicians from instances of burnout, compassion fatigue, and mental illness [19,20]. Furthermore, contemporary research suggests that while some individuals may possess an innate resilience, others have learned to develop and maintain a high degree of resilience through experience and learning [21]. Therein presents the opportunity for clinicians to identify means to cultivate and replenish resilience, in order to enhance psychological well-being.
Of the factors thought to contribute to resilience, mindfulness has increasingly gained attention in recent years [22,23,24]. Conceptualised as an intentional state of awareness, mindfulness concerns the process of bringing one’s attention to the present moment, in a non-judgmental and accepting manner [25]. When contemplating the potential benefits of mindfulness, Richardson [26] argued that a willingness to attend to unpleasant stimuli and events might encourage growth and adaptive reintegration; elements considered fundamental to resilience [27,28]. Contemporary research appears to support this assertion with positive correlations found between mindfulness and resilience [29]; distress tolerance [30], emotion regulation skills [31], and psychological flexibility [32]. Accordingly, various psychotherapeutic interventions incorporate a significant mindfulness component and are widely accepted as effective in the treatment of a range of psychological conditions [33,34].
Mindfulness-based interventions (MBIs) have demonstrated some value in increasing resilience [35,36], preventing burnout and compassion fatigue [37], and fostering psychological well-being [34,38]. Shapiro et al. [39] conducted one such study, using a randomised-controlled trial to assess an eight week mindfulness-based stress reduction program (MBSR; [25]) in human service professionals. Whilst the results demonstrated preliminary evidence for the potential of mindfulness interventions to reduce work-related stress and burnout among human service professionals, a small sample size limited the generalisability of these results. Additionally, this work did not consider resilience or other factors that might mediate treatment outcomes.
Several authors have called for the appropriate analysis of the mechanisms of change within such programs, rather than simply reporting variations in symptomology [40,41]. This issue is particularly salient in studies of MBIs as mindfulness practices are seldom used as a stand-alone intervention. As a result, it is often not possible to infer whether the beneficial outcomes of MBIs are in fact due to increased levels of mindfulness or other simultaneous therapeutic elements [42]. Investigating the mediators of interventions that target burnout and compassion fatigue may also allow an assessment of how such interventions are effective, and how they may be improved.
1.1 Aims and Hypotheses
The primary aim of this study was to examine the efficacy of a mindful-awareness and resilience skills training (MARST) program to enhance mindfulness and resilience, as a means of increasing psychological well-being and compassion satisfaction, and alleviating burnout and compassion fatigue in human service professionals. Furthermore, in response to calls for research of this nature to address the factors which mediate experimental outcomes, the current research investigates the indirect effect of the MARST intervention on burnout and compassion fatigue, through changes in mindfulness and resilience.
On the basis of the presented research, the following hypotheses were formulated. Hypothesis one, pertaining to short-term intervention effects, predicts that at post intervention the MARST group will report significantly higher levels of mindfulness, resilience, compassion satisfaction and psychological well-being, and significantly lower levels of burnout and compassion fatigue, compared to the control group. Hypothesis two predicted that the intervention outcomes outlined in the first hypothesis will be maintained at one month post-intervention. Hypothesis three, predicted that increased levels of resilience and psychological well-being, as a result of participation in the MARST group, will be mediated by increased mindfulness. Hypothesis four predicted that reductions in compassion fatigue, as a result of participation in the MARST group, will be mediated by increased mindfulness and resilience. Hypothesis five predicted that reductions in burnout, as a result of participation in the MARST group, will be mediated by increased mindfulness and resilience. That is, mindfulness and resilience will emerge as significant unique mediators, and together as a group of mediators, of the impact of the MARST intervention on compassion fatigue and burnout.
2. Method
2.1 Participants
A sample of 50 human service professionals was recruited from a not-for-profit community and family services organisation. The professionals provide a range of services for children, young people and families including: counselling, family intervention and support, live-in home services for mothers and babies, and community engagement and development programs. Of the initial sample, 46 participants returned baseline data and met inclusion criteria (i.e., >18 years of age, working with clients directly and not engaged in professional psychological intervention at the time of recruitment). Table 1 presents the participant demographics.
The majority of participants reported that they did not practice mindfulness meditation at the time of recruitment (n = 25; 54.3%) and had not previously attended training in mindfulness meditation (n = 26; 56.5%). Based on random assignment, a total of 25 participants in the MARST group and 21 participants in the control group completed baseline and post-intervention data. A total of 41 human service professionals completed one month follow-up measurement, comprised of 23 and 18 participants from the MARST and control groups, respectively.
Table 1 Participant demographics.
|
Variables |
|
N |
% |
|
Age
Gender
Education
Employment status |
24 - 64 (M = 42, SD = 10.58)
Male Female
Bachelor Postgraduate Other
Full-Time Part-Time |
46
9 37
22 14 10
36 10 |
100
19.6 80.4
47.8 30.4 21.7
78.3 21.7 |
2.2 Materials
Demographic Questions. Participants were asked to supply demographic information for the purpose of describing the sample. Participants indicated their age, gender, education, employment status, involvement in current meditative practices, and participation in past mindfulness-based training programs or retreats.
Mindfulness. Self-reported mindfulness was assessed with the Five Facet Mindfulness Questionnaire (FFMQ; [43]). The FFMQ is a 39-item measure of five distinct skill areas cultivated by the practice of mindfulness: observing, describing, acting with awareness, non-reactivity, and non-judging. Items are measured on 5-point Likert scales (1 = never or very rarely true to 5 = very often or always true). The FFMQ identifies five subscale scores and a total FFMQ; with higher scores reflecting greater mindfulness [43]. Research has shown the FFMQ to be a valid and reliable measure of the skills cultivated by the practice of mindfulness, both in long-term meditators and in novices [44]. The measure has shown adequate internal consistency, with Cronbach’s alpha coefficients ranging from .73 for non-reactivity to .91 for describing [45]. In the present study, the Cronbach alpha value for total FFMQ was .87.
Resilience. The Resilience Quotient Scale (RQS; [46]) is a 60-item measure of an individual’s level of resilience, based on seven factors of resilience: emotion regulation, impulse control, causal analysis, self-efficacy, realistic optimism, empathy, and reaching out. Participants respond on 6-point scales (1 = not at all true to 5 = very true or often true, and 6 = don’t know) yielding total scores across each of the seven factors and an overall resilience quotient (RQ). Higher scores on each of the scales indicate a higher endorsement of that factor of resilience and a higher RQ indicated a higher level of resilience. The RQS is a valid and psychometrically sound instrument with established evidence of criterion and predictive validity [46]. Adequate internal consistency of the RQS was demonstrated in the present study with a Cronbach’s alpha of .83.
Compassion Fatigue, Burnout and Compassion Satisfaction. The Professional Quality of Life Scale - Fifth Edition (ProQOL-V; [47]) is a 30-item measure of compassion fatigue, burn-out and compassion satisfaction in those who work with traumatised populations. Compassion fatigue has been defined as a psychological syndrome resulting from work-related secondary exposure to extremely stressful events [48]. Items are measured on a 5-point scale (1 = never, 2 = rarely, 3 = sometimes, 4 = often and 5 = very often) with the three distinct constructs yielding independent totals. Validity evidence for the ProQOL is based on several studies indicating that practitioners with higher levels of compassion fatigue or burnout perform in a manner consistent with the construct [16,49]. The Cronbach’s alpha values reported by Stamm [47] for the three scales were .82 for compassion satisfaction, .71 for burnout, and .78 for compassion fatigue. The current study identified adequate internal consistency with mean values for Cronbach’s alpha as .88 for compassion satisfaction, .83 for compassion fatigue, and .89 for burnout.
Psychological Well-Being. The General Well-Being Schedule (GWS; [50]) is an 18-item self-reported measure of psychological well-being and distress. The instrument addresses six dimensions of subjective well-being including: depression, anxiety, positive well-being, self-control, vitality and general health. As several items are reverse scored (i.e., items 1, 3, 6, 7, 9, 11, 15, and 16), 14 is subtracted from the total score, yielding a total range of scores from 0 to 110; lower scores represent distress and higher scores representing greater well-being [50]. The GWB is a valid and psychometrically sound instrument with evidence of test-rest reliability and high internal consistency [47,51]. The total GWB mean value of Cronbach’s alpha in the current study was .73
2.3 Procedure
This research was approved by the affiliated university ethics committee and gatekeeper approval was obtained from the relevant not-for-profit organisation. The recruitment process commenced with an invitation to attend an information seminar delivered by the principal investigator. Following the presentation, participants expressing interest in the study were provided with an explanatory statement and requested to complete the battery of questionnaires.
Participants were assigned to the MARST or control groups on the basis of an unpredictable, chance (random) process, using simple (unrestricted) randomisation. This process involved the generation of a table of random numbers and the authors assigned participants to the trial groups. The table of random numbers was generated using the random number generator from http://stattrek.com/statistics/random-number-generator.aspx Prior to disbursement, 50 pre-intervention questionnaire packages were assigned a number based on the table of random numbers to allocate prospective participants to either the MARST group or the control group. Of the 50 participants who volunteered for the study, a total of 25 MARST group, and 21 control group participants returned completed pre-intervention questionnaires. Repeat data were obtained from the intervention and control groups at post-intervention and at one month follow-up. Minimal attrition was realised at one month follow-up in both groups, due to absences as a result of sick and annual leave, time pressures and conflicting organisational commitments. As a result, 41 human service professionals completed one month follow-up measurement, comprised of 23 MARST group and 18 control group participants. The schedule of the research design and measurement of the MARST and control groups is depicted in Figure 1.
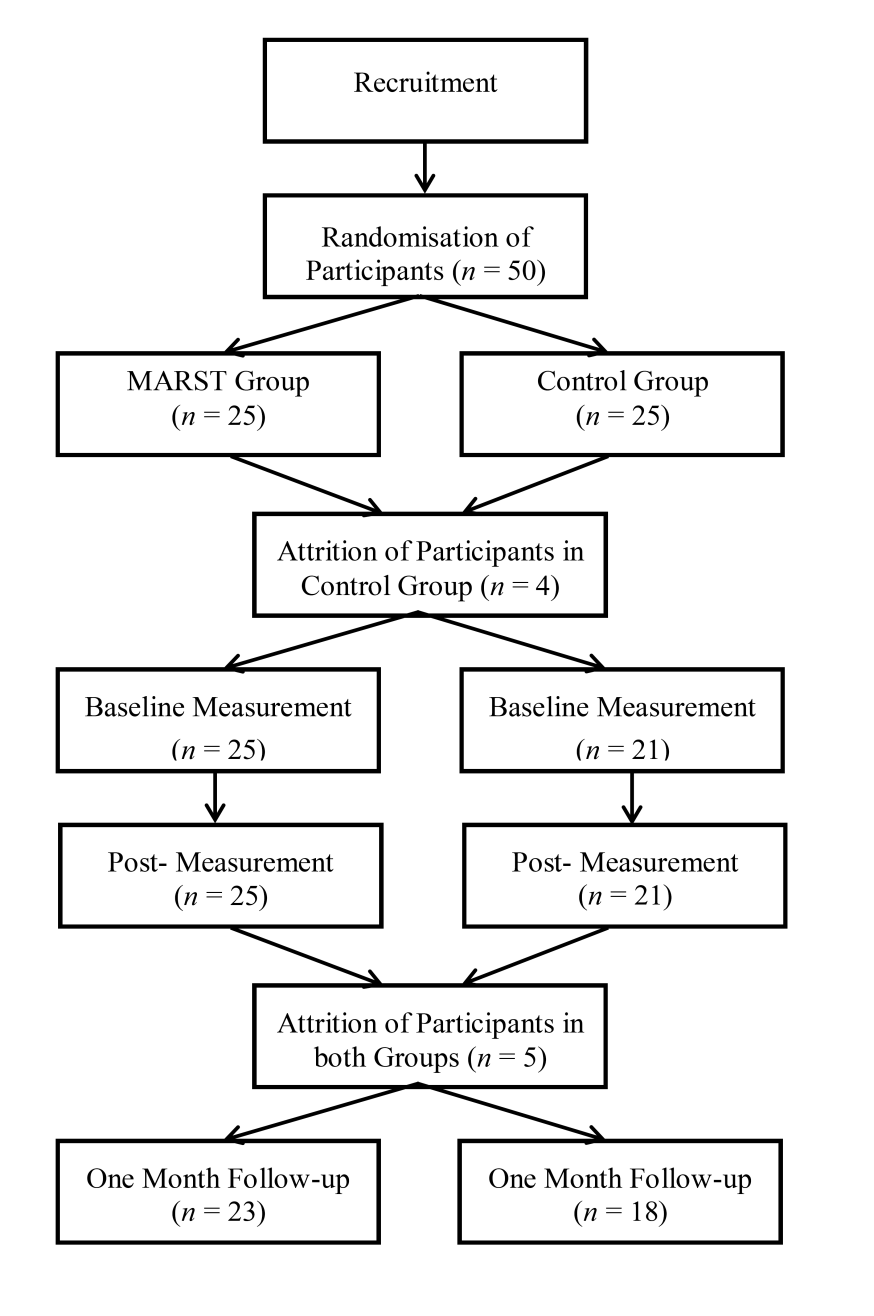
Figure 1 Schedule of research design and measurement for the mindful-awareness and resilience skills training group and the control group.
Mindful-Awareness and Resilience Skills Training (MARST). The MARST intervention involved three days (approximately eight hours) of training over three consecutive weeks. The program was facilitated by a clinical psychologist with some 20 years of experience utilising mindfulness-based approaches and training in mindfulness. The two co-facilitators had received training in mindfulness-based interventions as part of a Master’s Degree in Clinical Psychology and also regularly practiced formal meditation.
The MARST intervention teaches a set of core skills and strategies derived from the principles theoretically underpinning mindfulness-based cognitive therapy (MBCT; [52]) , mindfulness-based stress reduction (MBSR; [25]) and mindful self-compassion (MSC; [53]), and integrates some of the basic principles of cognitive behavioural therapy (CBT).
The mindfulness component of the program included training in formal (i.e., mindfulness of the breathe meditation, body-scan meditation and compassion meditation) and informal mindfulness practice (i.e., mindful walking, eating and posture exercises) with periods of extended silence. Approximately one hour of the program was devoted to teaching the basic cognitive behavioural ABC model however MARST aims to assist individuals to make changes in a different way to CBT. While CBT attempts to change unhelpful behaviour by modifying people's non-resilient thinking, MARST aims to assist individuals to learn to develop control over the processes that maintain the non-resilient thoughts through mindfulness training. Essentially, MARST aims to change the process of thinking, not just the content of the thoughts. Table 2 presents an overview of the structure and content of the MARST program.
Table 2 Overview of content of mindful-awareness and resilience skills training program.
|
Training Day |
Content |
|
Week 1 - Day One |
The MARST course objectives, content and structure. Psychoeducation on resilience and the cognitive-behavioural model. Introduction to the ABC model, strategies to develop resilient thinking. Introduction and practice of mindfulness and mindful-awareness skills. Home activities |
|
Week 2 - Day Two |
Review of home activities Introduction to mindfulness compassion meditation and mindful-awareness integration tool. Practice of formal and informal mindfulness meditation and exercises. Practice applying the mindful-awareness integration tool. Home activities |
|
Week 3 - Day Three |
Review of home activities Introduction to situational awareness and the map of mindful-awareness. Experiential exercises to develop resilient thinking. Practice of formal and informal mindfulness meditation and exercises. Practice applying the mindful-awareness integration tool. |
2.4 Design
A randomisation process was employed with one independent variable of two levels; the mindful-awareness and resilience skills training group (MARST) and no intervention (Control). The dependent variables for the study were resilience, mindfulness, compassion fatigue, burn-out and compassion satisfaction, and psychological well-being.
To determine group differences, multivariate analysis of covariance (MANCOVAs) were used to compare short-term (i.e., baseline to post intervention) and follow-up (i.e., baseline to one month follow-up) differences on each of the dependent variables; in combination with subsequent univariate analysis of variance (ANOVAs). In accordance with relevant research, baseline data and age were incorporated as covariates [54,55]. Next, the study incorporated a bootstrapping resampling procedure to explore the role of mindfulness in mediating the impact of participation in the MARST program on resilience and psychological well-being. Finally, multiple mediation analysis was conducted to consider the role of mindfulness and resilience, in mediating changes in compassion fatigue and burnout as a function of the MARST intervention.
3. Results
3.1 Multivariate Analysis of Covariance
Short Term Treatment Effects. A one-way between-groups MANCOVA was performed to investigate group differences for the six aforementioned dependent variables, immediately following the MARST intervention (i.e., post-intervention). The analysis included one independent variable of two levels; the MARST group and control (no intervention) group. Baseline scores on the dependent variables and participant age were used as covariates, to control for individual differences and reduce unexplained variance.
Preliminary checks were conducted to test assumptions of multivariate normality, linearity, univariate and multivariate outliers, and multicollinearity, with no violations noted. Covariates were judged to be adequately reliable for covariance analysis. A non-significant Box’s M indicated that the homogeneity of variance-covariance matrix assumption had not been violated. After adjusting for baseline scores and age, a significant multivariate main effect was found for group, F (6, 32) = 2.94, p <.05, Pillai’s Trace = .36; η2 = .36, power = .83.
Given the significant multivariate main effect, univariate analysis of variance (ANOVAs) for each dependent variable was assessed. Levene’s test of homogeneity was non-significant across all dependent variables, indicating the data set had equal variance across the sample. The results revealed significant univariate effects for group across the dependent variables; mindfulness, F(1, 44) = 5.92, p <.05, η2 =.14 ; resilience, F(1, 44) = 7.66, p <.01, η2 =.17; psychological well-being, F(1, 44) = 7.88, p <.01, η2 =.18; compassion satisfaction, F(1, 44) = 6.86, p <.05, η2 =.16; burnout, F(1, 44) = 12.19, p = .001, η2 =.25; and compassion fatigue, F(1, 44) = 12.46, p =.001, η2 = .25.
Table 3 displays the means and standard deviations for the dependent variables between groups, at baseline, post-intervention and one month follow-up. As noted in Table 3, the MARST group reported significantly higher levels of mindfulness, resilience, psychological well-being, and compassion satisfaction post-intervention, compared to the control group. Furthermore, the MARST group reported significantly lower levels of burnout and compassion fatigue, when compared with the control group immediately following the intervention. Thus, the results suggest that hypothesis one was supported.
Follow-up Treatment Effects. A one-way between-groups MANCOVA was performed to investigate group differences for the dependent variables, one month following the MARST intervention (i.e., follow up effects). The analysis included group allocation as the independent variable and the six dependent variables. Baseline scores on the dependent variables and participant age were used as covariates as per previous research [54,55].
Results of evaluation of assumptions of normality, linearity, univariate and multivariate outliers, reliability of covariates, and multicollinearity were considered satisfactory. Results showed a significant multivariate main effect was found for group, F (6, 27) = 2.92, p <.05, Pillai’s Trace = .39; η2 = .39, power = .81.
Given the significant multivariate main effect, univariate analyses of variance (ANOVAs) for each dependent variable were examined. Levene’s test was non-significant across all dependent variables, indicating homogeneity of variance. The results revealed significant univariate effects for group across the following dependent variables; mindfulness, F(1, 39) = 6.84, p <.05, η2 =.18; resilience, F(1, 39) = 16.75, p <.001, η2 =.34; psychological well-being, F(1, 39) = 5.19, p <.05, η2 =.14; burnout, F(1, 39) = 8.55, p <.01, η2 =.21; and compassion fatigue, F(1, 39) = 5.87, p <.05, η2 = .16. No significant difference was found between groups on measures of compassion satisfaction at one month follow-up, F(1, 39) = 18.73, p >.05, η2 =.02.
As shown in Table 3, the MARST group reported significantly higher levels of mindfulness, resilience and psychological well-being and significantly lower levels of burnout and compassion fatigue at one month follow-up compared to the control group. As differences in compassion satisfaction between groups were not statistically significant, hypothesis two was partially supported.
Table 3 Means and Standard Deviations of the Dependent Variables between Groups at Pre, Post and Follow-up.
|
|
MARST (n = 23) |
|
Control (n = 18) |
|||||||||
|
Variable |
Pre |
Post |
Follow-Up |
|
Pre |
Post |
Follow-Up |
|||||
|
M (SD) |
M (SD) |
M (SD) |
|
M (SD) |
M (SD) |
M (SD) |
|
|||||
|
Mindfulness |
138.60 (28.44) |
149.44 (20.12) |
154.04*(21.82) |
|
135.14 (20.69) |
136.19 (22.53) |
139.28 (21.25) |
|
||||
|
Resilience |
67.15 (9.32) |
70.17 (6.87) |
74.30***(7.01) |
|
66.11 (9.76) |
64.37 (12.21) |
64.72 (11.19) |
|
||||
|
Psychological Well-being |
70.96 (16.69) |
80.92 (11.20) |
80.22* (12.66) |
|
76.14 (14.84) |
73.62 (13.72) |
73.83 (15.39) |
|
||||
|
Compassion Satisfaction |
41.04 (6.24) |
42.12 (4.72) |
42.35 (5.60) |
|
40.38 (5.94) |
38.52 (7.25) |
39.61 (7.78) |
|
||||
|
Burnout |
20.20 (5.45) |
18.20 (3.42) |
18.09** (4.34) |
|
20.00 (6.12) |
21.62 (6.38) |
21.67 (6.49) |
|
||||
|
Compassion Fatigue |
18.56 (4.45) |
17.68 (3.59) |
17.17* (3.71) |
|
18.90 (5.21) |
21.76 (6.36) |
20.00 (7.57) |
|
||||
Note. * p<.05, ** p<.01, ***p<.001. MARST = mindful-awareness and resilience skills training (treatment group).
3.2 Simple Mediation Analysis: Bootstrap Resampling
Mediation analysis was conducted using a bootstrap resampling method which provides a formal significance test of the indirect effect (ab product; [56]).This procedure is a non-parametric multivariate extension of the Sobel test, recommended with studies of smaller sample sizes (i.e., n < 80) as it is considered to have higher power with reasonably controlled Type I error rate [57].
Within the current study, bootstrapping was accomplished by taking 5000 samples of the original sample size at post-intervention (n = 46) and computing the ab product for the mediator in each sample [56]. The point estimate of the indirect effect is the mean of the ab product over 5000 samples and the procedure yields a 95% confidence interval [56,57]. If the upper and lower limits of the confidence interval do not contain zero, the null hypothesis may be rejected and the indirect effect is significant [56].
The Indirect Effect of the MARST Intervention on Resilience, through Mindfulness. Mediation analysis was conducted to assess mindfulness as a potential mediator of improvements in resilience as a result of participation in the MARST intervention. The analysis included a dichotomous independent (predictor) variable; participation in the MARST group and no intervention (control) group, post-intervention mindfulness as the mediator, and post-intervention resilience as the dependent variable. As per previous research, baseline covariates where included in the analysis to increase the efficacy of estimating the direct and indirect effects [54,58]. Furthermore, due to the dichotomous nature of the independent variable, regression coefficients were reported in unstandardised form [59]. The analysis was conducted using SPSS macros for mediation analysis provided online at http://www.afhayes.com/spss-sas-and-mplus-macros-and-code.html#indirect.
Results indicated that participation in the MARST group (as opposed to the control group) was positively related to resilience (B = 5.00, SEB = 1.66, t(44) = 3.00, p <.01). It was also found that participation in the MARST group was positively related to increased mindfulness (B = 11.16, SEB = 4.35, t(44) = 2.56, p <.05). Lastly, results indicated that the mediator, mindfulness, was positively associated with resilience (B = .24, SEB = .05, t (44) = 5.11, p <.001). Figure 2 displays the mediation results and unstandardised regression coefficients.
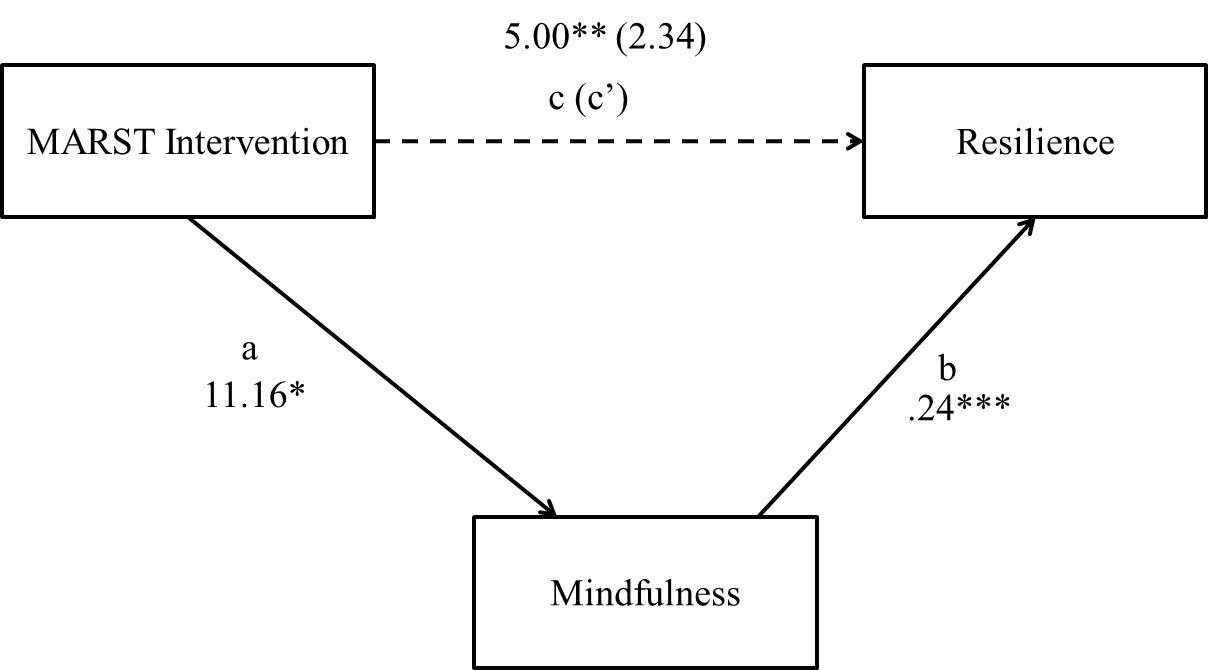
Figure 2 Indirect effect of MARST intervention on resilience, through mindfulness. Note. * p<.05, ** p<.01, ***p<.001. a = independent variable to mediator, b = mediator to dependent variable, c = total effect, c’ = direct (partial) effect.
As both the a-path and b-path were significant, mediation analysis based on 5000 bootstrapped samples using bias-corrected 95% confidence estimates was conducted [56,57]. Results confirmed the significant mediating role of mindfulness in the relationship between participation in the MARST group and resilience (B = 2.70, CI = .69 to 5.91). In addition, the results indicated that the direct effect of the MARST program on resilience became non-significant when controlling for the effects of mindfulness (B = 2.34, SEB = 1.41, t(44) = 6.39, p >.05), thus suggesting full mediation and support of hypothesis three.
The Indirect Effect of the MARST Intervention on Psychological Well-Being, through Mindfulness. Mediation analysis was conducted to assess whether improvements in psychological well-being as a result of participation in the MARST group, were mediated by increased mindfulness. Thus, the analysis included the independent variable of two levels; participation in the MARST group and no intervention (control) group, post-intervention mindfulness as the mediator, post-intervention psychological well-being as the dependent variable, and baseline scores as the covariates. First it was found that participation in the MARST group (as opposed to the control group) was positively related to psychological well-being (B = 8.76, SEB = 3.56, t(44) = 2.46, p <.05). It was then found that participation in the MARST group was positively related to increased mindfulness (B = 10.75, SEB = 4.61, t(44) = 2.33, p <.05). Next, results indicated that the mediator, mindfulness, was positively associated with psychological well-being (B = .38, SEB = .10, t(44) = 3.64, p <.001).
Mediation analysis using the bootstrapping method with bias-corrected confidence estimates was conducted and a 95% confidence interval of the indirect effect was obtained (5000 samples; [56,57]). Results of the mediation analysis confirmed the significant mediating role of mindfulness in the relationship between participation in the MARST group and psychological well-being (B = 4.07, CI = .61 to 8.43). The results also found that the direct effect of the MARST program on psychological well-being became non-significant when controlling for the effects of mindfulness (B = 4.66, SEB = 3.33, t(44) = 1.40, p >.05); indicating full mediation and support of hypothesis three. Figure 3 displays the results of the mediation analysis and unstandardised regression coefficients.
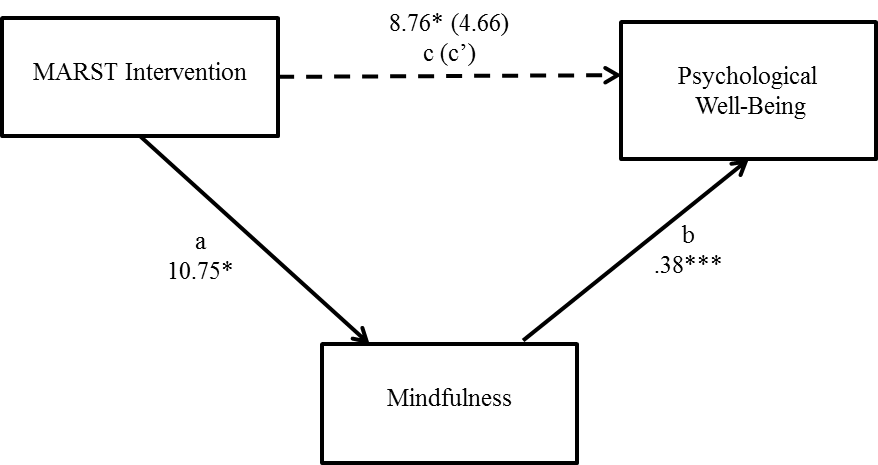
Figure 3 Indirect effect of MARST intervention on psychological well-being, through mindfulness. Note. * p<.05, ** p<.01, ***p<.001. a = independent variable to mediator, b = mediator to dependent variable, c = total effect, c’ = direct (partial) effect.
3.3 Multiple Mediation Analysis: Bootstrap Resampling
The Indirect Effect of the MARST Intervention on Compassion Fatigue, through Mindfulness and Resilience. To explore hypothesis four, that changes in mindfulness and resilience will mediate the impact of the MARST intervention on compassion fatigue, a bootstrapping resampling procedure that allows the simultaneous examination of multiple mediators was conducted [41]. In the current analysis, changes in mindfulness and resilience were entered as candidate mediators of the effects of participation in the MARST group (as opposed to the control group) on changes in compassion fatigue.
The results indicated that participation in the MARST group was negatively related to compassion fatigue, (B = -3.97, SEB = 1.50, t(44) = -2.65, p <.05). It was also found that participation in the MARST group was positively related to increased mindfulness (B = 11.16, SEB = 4.35, t(44) = 2.56, p <.05) and resilience (B = 5.00, SEB = 1.66, t(44) = 3.00, p <.01). Lastly, it was found that resilience was negatively associated with compassion fatigue (B = -.46, SEB = .15, t(44) = -3.13, p <.01), however changes in mindfulness were non-significant (B = -.04, SEB = .06, t(44) = -.63, p >.05). Figure 4 displays the results and unstandardised regression coefficients.
As the a-path and b-path were significant for the mediator, resilience, bootstrapping with bias-corrected confidence estimates was subsequently conducted with a 95% confidence interval of the indirect effect (5000 samples; [41]). Results of the mediation analysis confirmed the role of resilience in mediating the relationship between participation in the MARST group and reductions in compassion fatigue (B = -2.26, CI = -4.65 to -.83). Furthermore, the results indicated that the direct effect of the MARST group on compassion fatigue became non-significant when controlling for the effects of the mediators (B = -1.26, SEB = 1.38, t(44) = -.91, p = .37). However, as only resilience emerged as a unique individual mediator (specific indirect effect), hypothesis four was partially supported.
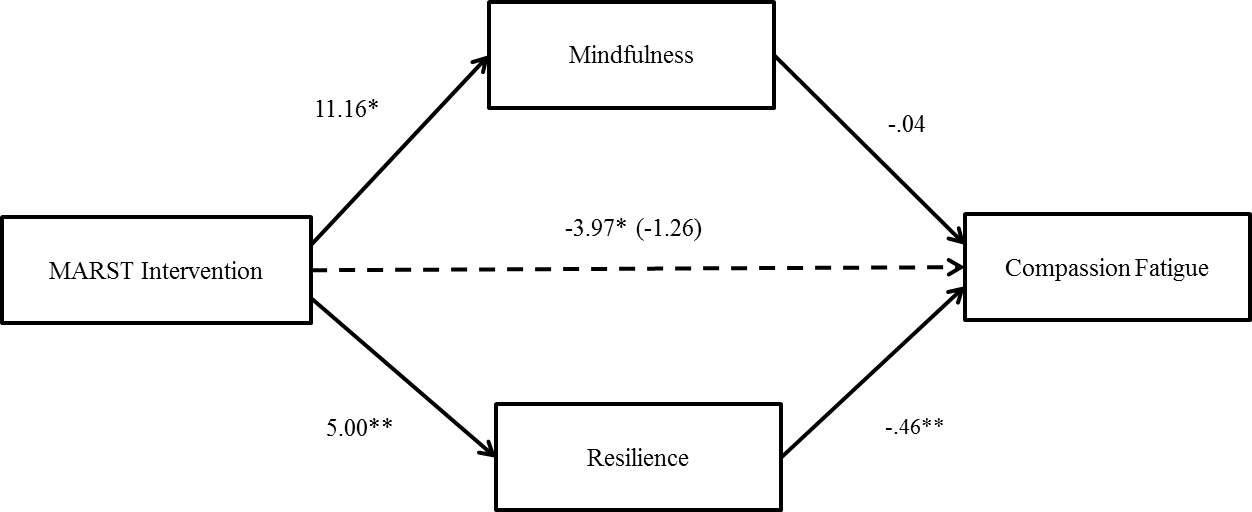
Figure 4 Mediation analysis of mindfulness and resilience as candidate mediators of the MARST intervention’s effects on changes in compassion fatigue. Note. * p<.05, ** p<.01, ***p<.001.
The Indirect Effect of the MARST Intervention on Burnout, through Mindfulness and Resilience. Changes in mindfulness and resilience were entered as candidate mediators of the effects of group participation (MARST intervention vs. control) on changes in burnout. The results indicated that participation in the MARST group was negatively related to burnout, (B = -3.16, SEB = 1.35, t(44) = -2.35, p <.05). It was also found that participation in the MARST group was positively related to increased mindfulness (B = 11.16, SEB = 4.35, t(44) = 2.56, p <.05) and resilience (B = 5.00, SEB = 1.66, t(44) = 3.00, p <.01). Next, it was found that the mediators, mindfulness (B = -.14, SEB = .05, t(44) = -3.05, p <.01) and resilience (B = -.26, SEB = .12, t(44) = -2.24, p <.05), were negatively associated with burnout.
Bootstrapping with bias-corrected confidence estimates was therefore conducted with a 95% confidence interval of the indirect effect (with 5000 samples; [41]). Results of the mediation analysis confirmed the independent mediating roles (specific indirect effects) of mindfulness (B = -1.48, CI = -3.82 to -.21) and resilience (B = -1.32, CI = -2.80 to -.25) in the relationship between MARST participation and reductions in burnout. Additionally, the results indicated that the direct effect of the MARST program on burnout became non-significant when controlling for the effects of the mediators as a group (B = -.31, SEB = 1.10, t(44) = -.28, p >.05), subsequently demonstrating full mediation and support of hypothesis five. Figure 5 displays the results of the mediation analysis and unstandardised regression coefficients.
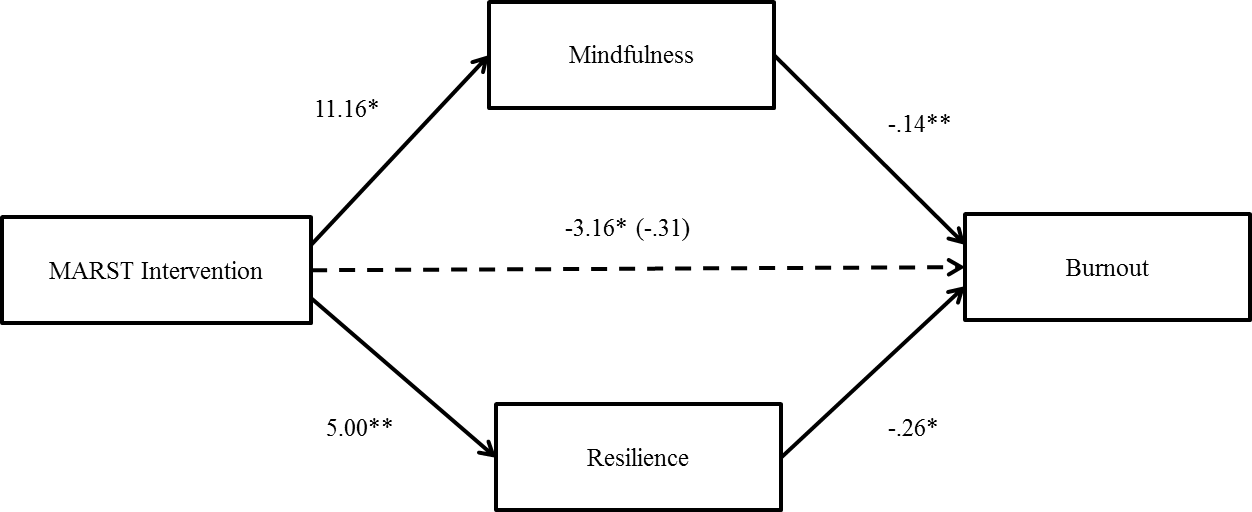
Figure 5 Mediation analysis of mindfulness and resilience as candidate mediators of the MARST intervention’s effects on changes in burnout. Note. * p<.05, ** p<.01, ***p<.001.
4. Discussion
To the authors’ knowledge, this was the first study to implement and evaluate a brief intensive mindfulness based program to cultivate resilience and mindfulness, as a means of increasing psychological well-being and reducing burnout and compassion fatigue, in human service professionals. To achieve this, the study examined the efficacy of a mindful-awareness and resilience skills training (MARST) program and sought to determine if treatment outcomes were mediated by increased levels of mindfulness and/or resilience.
The first and second hypotheses predicted that compared to the control group, MARST participants would report significantly higher levels of mindfulness, resilience, compassion satisfaction and psychological well-being, and significantly lower levels of burnout and compassion fatigue; immediately after and one month following the intervention. These effects were found across each of the variables, at both time intervals, with the exception of compassion satisfaction which failed to sustain self-reported improvements.
In agreement with authors that describe resilience as a dynamic and modifiable construct [20] this finding suggests that clinician resilience is indeed amenable to change and responsive to educational and cognitive transformational processes. The results also corroborate findings which suggest that mindfulness-based interventions (MBIs) may effectively replenish resilience [36,60] reduce states of burnout and traumatic stress [37,39], and improve psychological well-being [34,38]. Notwithstanding the non-significant finding of compassion satisfaction at follow up, the MARST program was effective in producing sustainable outcomes over time.
Although practitioners may require additional or supplementary intervention to ensure compassion satisfaction is maintained, improvements in mindfulness and resilience seemed to accumulate and develop with time. This result was indicated by larger proportions of variance attributable to the MARST group at one-month follow up; resilience (post = 17%; one month follow up = 34%) and mindfulness (post = 14%; one month follow up = 18%). In a similar observation, Pidgeon et al. [60] predicted that the development of mindfulness and resilience may mature with time, following an opportunity to practice the skills learnt. Should this assertion be justified, one might conceptualise growth in these areas as following a ‘snowball effect’, based on the maintenance of skills triggered by this brief intensive intervention.
Hypothesis three was supported and indicated that self-reported gains in resilience and psychological well-being, following participation in MARST, were fully mediated by increased mindfulness. This finding exemplifies the ability of human service professionals to build resilience and enhance their psychological well-being through interventions and practices which increase mindfulness. The mediating effect of mindfulness in influencing change in resiliency and psychological well-being is also consistent with previous studies which suggest that mindfulness is related to the development of skills that form the fundamental elements of resilience [27,28].
Hypothesis four and five predicted that reductions in compassion fatigue and burnout, as a result of MARST participation, would be mediated by increased mindfulness and resilience. Although resilience was found to mediate the relation between MARST and compassion fatigue, mindfulness was not a significant mediator of this effect. Both mindfulness and resilience were however found to mediate the relationship between MARST and self-reported burnout.
Interestingly, this result may add to the assumed path by which MARST influenced its outcomes. While mindfulness did not directly mediate MARST’s impact on compassion fatigue, increased mindfulness was found to mediate the relationship between the intervention and resilience, which in turn mediated change in compassion fatigue. This may suggest that participation in MARST led to increased levels of mindfulness, which resulted in increased resilience, which subsequently impacted upon reductions in compassion fatigue. Conversely, when considering clinical interventions for burnout among professionals, both mindfulness and resilience appear to be important unique therapeutic targets.
The noted mediation effect supports research which highlights the importance of personal qualities and characteristics in safeguarding against compassion fatigue and burnout [48]. According to third wave resilience research, increased mindfulness may provide the positive growth and cognitive transformational processes required to replenish resiliency factors [26]. The development of resilience would in turn safeguard professionals against the repeated exposure to traumatic material inherent to the human service professions [19]. Further to this, developing skills to cultivate mindfulness and replenish resilience may serve to protect clinicians from mental exhaustion and workplace disengagement, by providing additional resources and restoring the balance with occupational demands [13].
Nevertheless, a number of limitations must be considered when examining these results. First, attrition contributed to the small sample size which limits the generalisability of the findings. The sample was predominantly female, well-educated and recruited from the same not-for-profit organisation. A large percentage of participants also reported prior experience with mindfulness. Whilst exposure to mindfulness training among human service professionals is to be expected, the research may have appealed more so to those individuals that are open to this intervention. Future studies should include a larger sample recruited from more diverse educational and socioeconomic backgrounds, and multiple human service employers. The current study also involved a no intervention control and future studies would benefit from the use of an alternative intervention or waitlist control. In light of findings that mindfulness and resiliency skills may develop with time, additional longitudinal measurement may also assist researchers to examine this phenomenon further.
There are several implications of this work for future research. The findings contribute to an understanding of the factors which influence the development and maintenance of resilience, in addition to means of alleviating burnout and compassion fatigue among human service professionals. The study provides preliminary evidence for MARST as a brief, intensive intervention that may bolster psychological resources and safeguard against known job-related risk factors, prevalent among this occupational group. Results suggest that interventions which effectively increase mindfulness among human service professionals may result in the added benefits of increased resilience and subsequent reductions in instances of burnout and compassion fatigue. Although the findings are to be interpreted with some caution given the limitations of the study, they highlight the value of simultaneously examining multiple variables as mediators of the effects of mindfulness-based interventions.
Acknowledgments
The authors gratefully acknowledge the participation and support of Francis Klaassen and the staff at Mercy Family Services, without which the present study could not have been completed. The authors would also like to thank Breeana Souter for her assistance in co-facilitating the MARST program.
Author Contributions
Both authors contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript.
Funding
This research was financially supported by Mercy Family Services.
Competing Interests
The authors have declared that no competing interests exist.
References
- Angerer JM. Job burnout. J Employ Couns. 2003; 40: 98-107. [CrossRef]
- Stebnicki MA. Empathy fatigue: healing the mind, body, and spirit of professional counselors. Am J Psychiat Rehabil. 2007; 10: 317-338. [CrossRef]
- Brian E. Bride PhD L, MSW EW. Secondary traumatic stress in substance abuse treatment. J Teach Addict. 2006; 5: 5-20. [CrossRef]
- Figley CR. Treating compassion fatigue. Hoboken: Taylor and Francis; 2002.
- Rossi A, Cetrano G, Pertile R, Rabbi L, Donisi V, Grigoletti L, et al. Burnout, compassion fatigue, and compassion satisfaction among staff in community-based mental health services. Psychiatry Res. 2012; 200: 933-938. [CrossRef]
- Elwood LS, Mott J, Lohr JM, Galovski TE. Secondary trauma symptoms in clinicians: A critical review of the construct, specificity, and implications for trauma-focused treatment. Clin Psychol Rev. 2011; 31: 25-36. [CrossRef]
- Harr C. Promoting Workplace Health by Diminishing the Negative Impact of Compassion Fatigue and Increasing Compassion Satisfaction. Soc Work Christian. 2013; 40: 71-88.
- Figley CR. Compassion fatigue as secondary traumatic stress disorder: an overview. compassion Fatigue. New York: Brunner/Maze; 1995.
- Hegney DG, Craigie M, Hemsworth D, Osseiran-Moisson R, Aoun S, Francis K, et al. Compassion satisfaction, compassion fatigue, anxiety, depression and stress in registered nurses in Australia: study 1 results. J Nurs Manag. 2014; 22: 506-518. [CrossRef]
- Cunningham M. Impact of trauma work on social work clinicians: empirical findings. Soc Work. 2003; 48: 451-459. [CrossRef]
- Vanderlinden J, Vandereycken W. Trauma, dissociation, and impulse dyscontrol in eating disorders. New York: Brunner/Maze; 1999.
- Austin W, Goble E, Leier B, Byrne P. Compassion fatigue: the experience of nurses. Ethics Soc Welfare. 2009; 3: 195-214. [CrossRef]
- Demerouti E, Nachreiner F, Bakker AB, Schaufeli WB. The job demands-resources model of burnout. J Appl Psychol. 2001; 86: 499-512. [CrossRef]
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001; 52: 397-422. [CrossRef]
- Angerer JM. Job burnout. J Employ Couns. 2003; 40: 98-107. [CrossRef]
- Potter P, Deshields T, Divanbeigi J, Berger J, Cipriano D, Norris L, et al. Compassion fatigue and burnout: prevalence among oncology nurses. Clin J Oncol Nurs. 2010; 14: E56-62. [CrossRef]
- Seligman ME. Building resilience. Harv Bus Rev. 2011; 89: 100-106, 138.
- Edward KL. The phenomenon of resilience in crisis care mental health clinicians. Int J Mental Health Nurs. 2005; 14: 142–148. [CrossRef]
- Grafton E, Gillespie B, Henderson S. Resilience: the power within. Oncol Nurs Forum. 2010; 37: 698-705. [CrossRef]
- Jackson D, Firtko A, Edenborough M. Personal resilience as a strategy for surviving and thriving in the face of workplace adversity: a literature review. J Adv Nurs. 2007; 60: 1-9. [CrossRef]
- Phillips G. Resilience in practice interventions. Child Care Pract. 2008; 14: 45-54. [CrossRef]
- Breckman B. Mindfulness as a key resource for development and resilience. Nurs Stand. 2012; 26: 32. [CrossRef]
- Owen R. Facing the storm: using CBT, mindfulness and acceptance to build resilience when your world 1st ed. New York: Taylor and Francis; 2012.
- Rogers HB. Mindfulness meditation for increasing resilience in college students. Psychiat Ann. 2013; 43: 545-548. [CrossRef]
- Kabatzinn J. Mindfulness-based interventions in context: past, present, and future. Clin Psychol Sci Pract. 2003; 10: 144-156. [CrossRef]
- Richardson GE. The metatheory of resilience and resiliency. J Clin Psychol. 2002; 58: 307-321. [CrossRef]
- Feder A, Nestler EJ, Charney DS. Psychobiology and molecular genetics of resilience. Nat Rev Neurosci. 2009; 10: 446-457. [CrossRef]
- Haglund ME, Nestadt PS, Cooper NS, Southwick SM, Charney DS. Psychobiological mechanisms of resilience: relevance to prevention and treatment of stress-related psychopathology. Dev Psychopathol. 2007; 19: 889-920. [CrossRef]
- Mirkova AM. Investigation of the Relationship between Resilience, Mindfulness, and Academic Self-Efficacy. Open J Soc Sci. 2013; 1: 1-4.
- Feldman G, Dunn E, Stemke C, Bell K, Greeson J. Mindfulness and rumination as predictors of persistence with a distress tolerance task. Pers Individ Dif. 2014; 56: 154-158. [CrossRef]
- Lutz J, Herwig U, Opialla S, Hittmeyer A, Jancke L, Rufer M, et al. Mindfulness and emotion regulation--an fMRI study. Soc Cogn Affect Neurosci. 2014; 9: 776-785. [CrossRef]
- Masuda, Akihiko, Tully, Erin C. The role of mindfulness and psychological flexibility in somatization, depression, anxiety, and general psychological distress in a nonclinical college sample. J Evid-Based Complement Altern Med. 2012; 17: 66-71. [CrossRef]
- Eberth J. The effects of mindfulness meditation: a meta-analysis. Mindfulness. 2012; 3: 174-189. [CrossRef]
- Keng SL, Smoski MJ, Robins CJ. Effects of mindfulness on psychological health: a review of empirical studies. Clin Psychol Rev. 2011; 31: 1041-1056. [CrossRef]
- Pidgeon AM, Ford L, Klaassen F. Evaluating the effectiveness of enhancing resilience in human service professionals using a retreat-based Mindfulness with Metta Training Program: a randomised control trial. Psychol Health Med. 2014; 19: 355-364. [CrossRef]
- Stanley EA, Schaldach JM, Kiyonaga A, Jha AP. Mindfulness-based mind fitness training: a case study of a high-stress predeployment military cohort. Cogn Behav Pract. 2011; 18: 566-576. [CrossRef]
- Geller R, Krasner M, Korones D. Clinician self-care: the applications of mindfulness-based approaches in preventing professional burnout and compassion fatigue (336). J Pain Symptom Manag. 2010; 39: 366-366. [CrossRef]
- Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003; 84: 822-848. [CrossRef]
- Shapiro SL, Astin JA, Bishop SR, Cordova M. Mindfulness-based stress reduction for health care professionals: results from a randomized trial. Int J Stress Manag. 2005; 12: 164-176. [CrossRef]
- Kraemer HC. Toward non-parametric and clinically meaningful moderators and mediators. Stat Med. 2008; 27: 1679-1692. [CrossRef]
- Preacher KJ, Rucker DD, Hayes AF. Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivariate Behav Res. 2007; 42: 185-227. [CrossRef]
- Thompson RW, Arnkoff DB, Glass CR. Conceptualizing mindfulness and acceptance as components of psychological resilience to trauma. Trauma Violence Abuse. 2011; 12: 220-235. [CrossRef]
- Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. 2006; 13: 27-45. [CrossRef]
- Baer RA. Measuring mindfulness. Contemp Buddhism. 2011; 12: 241-261. [CrossRef]
- de Bruin EI, Topper M, Muskens JG, Bogels SM, Kamphuis JH. Psychometric properties of the Five Facets Mindfulness Questionnaire (FFMQ) in a meditating and a non-meditating sample. Assessment. 2012; 19: 187-197. [CrossRef]
- Reivich K, Shatte A. The resilience factor: Seven essential skills for overcoming life’s inevitable obstacles. New York: Broadway Books; 2002.
- StammBH. The concise ProQOL manual [Internet]. 2013.
- Stamm BH. The ProQOL Manual: The professional quality of life scale: compassion satisfaction, burnout & compassion fatigue/secondary trauma scales. Baltimore: Sidran Press; 2005.
- Lauvrud C, Nonstad K, Palmstierna T. Occurrence of post traumatic stress symptoms and their relationship to professional quality of life (ProQoL) in nursing staff at a forensic psychiatric security unit: a cross-sectional study. Health Qual Life Out. 2009; 7: 31. [CrossRef]
- Mcdowell I. Measuring health: a guide to rating scales and questionnaires. Oxford University Press; 2006. [CrossRef]
- Taylor JE, Poston WS, Haddock CK, Blackburn GL, Heber D, Heymsfield SB, et al. Psychometric characteristics of the General Well-Being Schedule (GWB) with African-American women. Qual Life Res. 2003; 12: 31-39. [CrossRef]
- Segal ZV, Williams JMG, Teasdale JD. Mindfulness-based cognitive therapy for depression: A new approach to preventing relapse. New York: Guilford Press; 2002. (p. 351).
- Germer CK, Neff K. The mindful self-compassion training program. 2013: 365-396.
- Mayers A. Introduction to statistics and SPSS in psychology. Chemical Communications. 1966; 13: 416-417.
- Van Breukelen GJ, Van Dijk KR. Use of covariates in randomized controlled trials. J Int Neuropsych Soc. 2007; 13: 903-904. [CrossRef]
- Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004; 36: 717-731. [CrossRef]
- Mackinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behav Res. 2004; 39: 99. [CrossRef]
- Ten Have TR, Joffe MM. A review of causal estimation of effects in mediation analyses. Stat Methods Med Res. 2012; 21: 77-107. [CrossRef]
- Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York: Guilford Publications; 2013. (p. 335-337).
- Pidgeon A, Keye M. Relationship between resilience, mindfulness, and psychological well-being in university students. Int J Liber Arts Soc Sci, 2014; 2: 27-32.
