

Meditation as an Intervention for Health: A Framework for Understanding Meditation Research
Marcel Allbritton 1 ![]() , Carrie Heeter 2, *
, Carrie Heeter 2, * ![]()
- Core Resonance Works, New Orleans, USA
- Michigan State University, East Lansing, USA
* Correspondence: Carrie Heeter![]()
Academic Editors: Sok cheon Pak, Soo Liang Ooi
Special Issue: Health Benefits of Meditation
Received: July 30, 2018 | Accepted: October 8, 2018 | Published: October 9, 2018
OBM Integrative and Complementary Medicine 2018, Volume 3, Issue 4 doi: 10.21926/obm.icm.1804025
Recommended citation: Allbritton M, Heeter C. Meditation as an Intervention for Health: A Framework for Understanding Meditation Research. OBM Integrative and Complementary Medicine 2018; 3(4): 025; doi:10.21926/obm.icm.1804025.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
We propose a framework for understanding meditation that can support greater scientific rigor in reporting meditation research, and selecting meditation health interventions. There is no consistent and thorough framework for describing meditation research interventions. This impedes rigor of meditation research design and interpretation of findings. This also limits meaningful comparisons across research studies. The audience for this article includes researchers, meditation experts, healthcare professionals, and those with interest in meditation. The framework describes the key components of a meditation intervention. We also discuss how meditation can effect individuals differently, and provide suggestions for describing the qualifications of the expert who designed the meditations in an intervention. The meditation framework supports (1) comparing different meditation interventions, and (2) understanding how meditation interventions lead to outcomes. We provide examples from a Yoga Therapy perspective of meditation (our domain of expertise), and from published research on meditation to illustrate applications of the meditation framework. The meditation framework provides a way of characterizing meditation interventions by distinguishing seven essential components. The first four components describe the meditation session (individual, object, experience, and immediate effects). Approach describes the foundation and source of a meditation practice. The outcome component represents both intended goals or reasons for prescribing the meditation intervention and other longer term effects that may occur. The engagement component refers to duration, spacing and frequency of doing the practice and quality of attention. These seven components can be applied to any type of meditation intervention. We explain the components of the framework and then offer examples. Our goal is to express the importance of having a framework for describing components of meditation across systems of knowledge and methods of application. We hope this article begins a dialogue with experts in other forms of meditation interventions, as they apply, adapt and respond to the proposed framework.
Graphical abstract
Keywords
Meditation; yoga; meditation intervention
1. Introduction
Meditation interventions have become increasingly popular to support health, healing, and well-being. There are many different approaches, systems, and definitions of meditation. This creates challenges for rigorous study of meditation. We propose a framework for describing meditation interventions regardless of the approach or type of meditation researched. The framework provides a vocabulary for comparing and contrasting findings relative to different types of meditation interventions. The meditation framework can help inform research design and interpretation of findings in meditation research. The framework also supports greater scientific rigor in conducting meditation intervention research, and selecting meditation health interventions. The audience for the article includes researchers, meditation experts, healthcare professionals, and those with interest in meditation.
There are no consistent and rigorous standards for describing meditation research interventions. This impedes rigor of meditation research design and interpretation of findings. This also limits meaningful comparisons across research studies. Studies of meditation interventions for health often are rigorous in sample selection, sample size, measurement scales, and statistical analysis. And yet, the meditation intervention – the experimental manipulation – is inadequately characterized and reported.
Both authors are experts on meditation and trained researchers with PhDs. Our experience and background in meditation is from the Viniyoga perspective of Yoga and Yoga Therapy. Our goal is to express the importance of having a broad, consistent framework for describing meditation interventions across systems of knowledge and methods of application. Researchers can use this framework as they plan, describe, and evaluate meditation interventions.
2. A Framework of Meditation
Research publications about meditation interventions often do not adequately describe the intervention. More detail would help readers understand what was studied and enable researchers to interpret and build upon prior research. The framework we propose can be applied to any kind of meditation intervention. As stated previously, the framework can be helpful for the design of the intervention, and the interpretation and comparisons of meditation research.
There are many different approaches, systems, and definitions of meditation. The 2012 National Health Interview Survey’s question about meditation listed four kinds of meditation (mantra, mindfulness, spiritual, and meditation as part of other practices) and provided 12 specific examples (Transcendental Meditation, Relaxation Response, Clinically Standardized Meditation, Vipassana, Zen Buddhist meditation, mindfulness-based stress reduction, mindfulness-based cognitive therapy, centering prayer, contemplative meditation, Yoga, Tai Chi, and Qigong) [1]. This complex diversity of meditation practices, goals, and systems of knowledge creates challenges for rigorous study of meditation.
Taxonomies are one approach to making sense of meditation. Taxonomies have been used to classify styles of meditation based on the object of meditation and accompanying neurological processes during meditation. For example, Focused Attention (on a chosen meditation object) differs from Open Monitoring (of moment to moment experience) [2] and from Automatic Self-Transcendence (the absence of focus or effort) [3]. Another taxonomy separates consideration of the meditation process from three types of altered state (Cognitive, Affective, and Null) that can be achieved while meditating [4].
Our framework is not a classification taxonomy. We argue that it is essential when reporting on a meditation intervention to fully describe the intervention along all of the components. It is useful to apply taxonomic classifications. However, details related to the components of meditation are essential to include so that others can understand the intervention and potentially apply their own taxonomies.
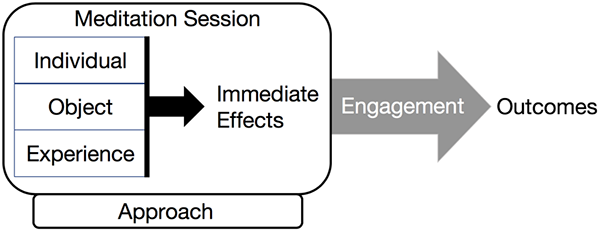
We conceptualize meditation as attention-based practices that have an immediate effect on the human system and lead to longer term outcomes. The framework describes the key components of any given meditation intervention and provides a vocabulary. The meditation framework supports (1) comparing different types of meditation interventions, and (2) understanding how meditation interventions lead to effects.
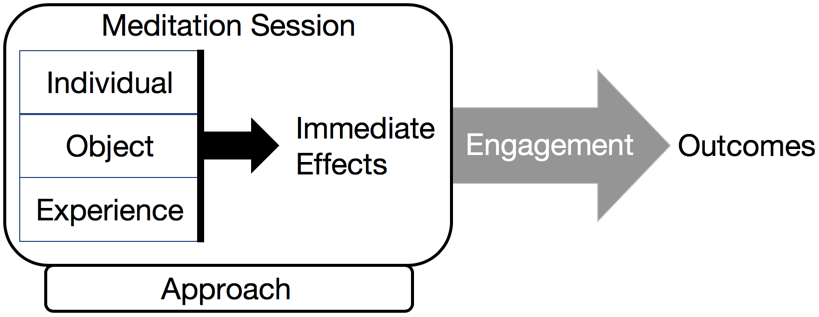
Figure 1 Meditation framework.
Our meditation framework, Figure 1, provides a way of understanding meditation by situating essential components. The first four (individual, object, experience, and immediate effects) are components of a meditation session. Approach describes the source or body of knowledge underlying a meditation practice. Longer term outcomes occur outside of the meditation session and are usually the result of repeated practice over time. Engagement refers to quality of attention, duration, spacing and frequency of doing the practice. These seven components can be applied to any type of meditation. We will explain the components of the framework and then offer examples.
3. The Meditation Session: Individual, Object, and Experience
In every meditation, a given individual is interacting with an object, in some way, and having an experience. Meditation research is conducted on populations (such as novice meditators, veterans with PTSD, or Buddhist monks) whose characteristics impact the process and effects of meditation. Beyond population differences, the effects of the meditation will vary from individual to individual and from session to session within an individual.
When describing a meditation intervention, we argue that it is important to describe the meditation object or objects used in the meditation sessions in order to understand the meditation intervention. We include object as a distinct component of the framework because of its importance and utility in characterizing and defining a meditation practice. The object of meditation refers to where the attention is placed during the meditation.
An object of meditation can be almost anything – a mantra, something in nature, an idea, god, nothingness, or self-observation. In open attention meditation, the object of meditation is less tangible – such as observing sensations and thoughts as they arise, without engaging with or judging them [2]. Simply labeling a meditation intervention based on a meditation taxonomy (such as focused attention or open monitoring) without detailing the meditation object limits understanding the current study and limits future comparative analyses. It is important to describe what a participant is directing their attention toward as part of characterizing meditation.
When reporting meditation research, it is important that the experience of the meditation be described. The object of meditation succinctly summarizes the attentional goal of the meditation session -- where the attention is placed. Experience refers to the what the individual does with their body, breath, and mind during the meditation. Experience includes any actual instruction or guidance, how the guidance is delivered, and the context of the meditation session. The instructions may be intrinsic, where the meditator directs herself or there may be extrinsic guidance by a meditation teacher. Guidance of a meditation experience may be delivered by a teacher who is physically present, a recording of instructions given throughout the meditation session, or even written instruction. Is the meditation delivered by an in-person teacher? In a group class or one-on-one? Is technology involved, such as an online class, smartphone app or web site? The many possible variations in how meditation is delivered may influence the experience of meditating as well as the effects.
Context is another aspect of experience. In what context is the study participant engaging in meditation? Are they in a research laboratory? At a meditation center for a week-long retreat? In a group yoga class? In a classroom or MBSR program with other people? At home?
4. Immediate Effects
In a meditation session, the individual has an experience that includes directing their attention toward an object. That experience results in an immediate effect on the human system (body, breath, mind, and emotions). Immediate effects are changes that occur during or immediately upon completion of a meditation session. Immediate effects include insights that arise during meditation and enhanced mental or affective states [4].
Some of the immediate effects -- the changes of the human system -- can easily be measured. For example, biometric data can indicate the physiological change in breath rate, heart rate, heart rate variability, blood pressure, cortisol levels, inflammation, interoceptive neural network activation, and characteristic EEG brainwave patterns. Immediate effects of meditation include physiological, psychological, and psychosocial changes. For example, health-related immediate effects can include a sense of calm and decreased feelings of anxiety. Immediate effects are easier to attribute to meditation than longer term effects because they occur during and/or immediately after the meditation. The timeframe is finite and the causal link is often more direct.
Immediate effects are interesting and important, but they are not the motivation for practicing, prescribing, or studying meditation. Lowering blood pressure during a 20 minute meditation session doesn’t matter very much if the effect occurs only during meditation, dissipates rapidly, and the human system returns to its original state.
5. Approach
Approach is the source of the meditation. Approach refers broadly to the tradition or system of knowledge a meditation intervention is based on. It is essential that the specific foundation of the meditation be referenced and cited in the research. Using vague titles like Yoga or Buddhism without mentioning specific bodies of knowledge, specific teachers, or describing specific techniques does not reflect scientific rigor [5]. The reader should be able to look up the body of knowledge that the meditation originated from. If the meditation did not originate from a specific body of knowledge, then it is important to describe the methods or techniques used in the meditation.
Many of the forms of meditation practiced in the west today have roots in ancient bodies of knowledge such as Buddhism and Yoga [6,7]. Endless variations exist, interpreted and adapted by individual teachers [8,9]. Some meditation approaches connote very specific meditation practices (such as Transcendental Meditation [10] or Kriya Yoga [11]). Mindfulness meditation was secularized and adapted for the West by Jon Kabat Zinn as part of Mindfulness Based Stress Reduction (MBSR) [12] and by other students of Buddhism in other meditation interventions. Mindfulness meditation also now has a clinical definition, as Western science studies and appropriates the original concepts [8,13].
If the meditations have roots in a tradition but have been adapted, it is important to identify the tradition and characterize the adaptation. The foundation underlying the meditation should be explicit and apparent. If the foundation is not stated explicitly and clearly, at a minimum, the methods and techniques should be clearly described.
Programs like MBSR and apps like Headspace draw from several traditions as well as other sources of knowledge and the developers’ personal experience. For example, Jon Kabat-Zinn developed MBSR based on his training in Zen Buddhism and Yoga; however, MBSR meditations are not presented to participants as Buddhist [14]. A study participant doing a meditation may not care or need to know the roots of the practice. However, researchers studying a meditation intervention should include information about the origin of the meditation methods and techniques in publications.
As we mentioned earlier, this diversity in meditation interventions complicates research on meditation. The practices that are coherently and consistently grounded in a system of knowledge can draw upon that system to develop theories and mechanisms of effect. For example, scientists have proposed theoretical mechanisms for the effects of Yoga [15,16,17] and of mindfulness meditation [18,19]. Meditation interventions that are a combination of different approaches are more complicated to study or interpret. But characterizing the meditation intervention using our framework may be helpful.
6. Outcomes
Goals or intended outcomes of a meditation intervention for health should be stated clearly in meditation research. Outcomes refer to how the meditation changes the human system so that it functions or operates differently in some desired direction as a result of the meditation practice. We suggest that it is helpful to think about meditation in an outcome-based way. In other words, why is meditation being used as an intervention? What are the expected outcomes of the meditation? The intended outcomes may be general or specific, but they should be stipulated. Otherwise, you have no way of assessing whether or not the meditation was an effective intervention.
The goal of meditation is to change the human system in the direction of a desired outcome. A distinction that our meditation framework makes is that meditation interventions are not just about the individual meditation session. It is very helpful when meditation research provides a theoretical explanation of how the meditation session (individual, object, experience, and immediate effects) leads to intended outcomes.
Examples of meditation outcomes for health include easing symptoms of anxiety, improved response to stress, improved functioning of immune system, support for sleep and reduction of insomnia, support for pain management, reduced mind wandering and dispositional mindfulness. Meditation has also been studied for other mental health, musculoskeletal and neurological, endocrine, and cardiorespiratory outcomes. The possibilities for meditation outcomes are vast.
Meditation interventions for health are prescribed to achieve particular or general intended outcomes. These intended outcomes are not the only outcomes that occur from practicing meditation. For example, the original goals for practicing Yogic, Buddhist, and other contemplative meditation related to self-transformation, equanimity, reducing suffering, and/or deepening spiritual connection. In other words, these practices did not originate to treat specific or health-related goals. In addition to intended health outcomes many known and unknown ancillary neurological, physiological and psychological changes to the human system occur as a result of practicing meditation.
7. Engagement
Meditation can have effects in different ways. Meditating has immediate effects on the human system at the time of the meditation session. But meditation is practiced, prescribed, and studied not simply for immediate effects but primarily because of the potential powerful and longer lasting changes that repeated meditation can bring about in the human system.
Meditation practices can have effects that extend beyond the practice session. Those effects are often gradual and cumulative, as a result of engagement. In the meditation framework, engagement refers to the duration, intensity, and spacing of meditation sessions [20] (such as how often, for how long, over what time period). The immediate effects and the outcomes of a meditation are influenced by how often and for how long an individual meditates. It is important for research to clearly describe the frequency of meditation sessions. This way, the relationship between engagement and outcomes can be better understood.
We use the term “engagement” rather than dose to emphasize that engagement also refers to the quality of attention during a meditation session. Sitting on a meditation cushion and playing a 20 minute breath awareness meditation audio while the mind is thinking about what to say to a co-worker or composing a grocery list impedes the effectiveness of meditation. The capacity to direct attention during meditation increases with practice. Quality of attention contributes to the effect and effectiveness of meditation.
Research and ancient and modern practice guidelines strongly support the proposition that deeper, longer lasting benefits of meditation arise from repeated sustained practice over a period of time [21]. Indications are that the benefits continue to grow the longer meditation is practiced. It is not only that the person develops the skill of meditating. It is that effectiveness in meditation is, to a degree, based on the action of engaging in the meditative experience repeatedly and with regularity over time. In other words, many of the effects of meditation emerge at least in part due to the amount of exposure the individual has to the meditation practice.
Powerful, systemic changes in the human system occur as a result of doing the meditation practice over time. When a yoga therapist meets with a client, as part of the session, the therapist observes the client doing their practice. Thus, with every individual client, yoga therapists observe the effects of meditation on an individual over time. Recognizing the importance of engagement, clinical studies of meditation typically involve a minimum of 6 to 8 weeks of daily home practice. While 6-8 weeks constitutes a level of engagement, this duration represents novices who have just begun to develop a meditation practice. Different or more sustained outcomes may require intermediate levels of engagement (3 to 12 months). Studies of long term meditators consider years [22,23,24] of daily practice.
Research and practices strongly support the proposition that deeper, longer lasting benefits of meditation arise from repeated sustained practice [21]. Indications are that the changes in how the human system functions continue to occur the longer meditation is practiced. It is not only that the person develops the skill of meditating. It is that effectiveness in meditation is, to a degree, based on the action of engaging in the meditative experience repeatedly and with regularity over time.
8. Meditation Effects Individuals Differently
We cannot assume that a meditation experience that is delivered in a consistent way will impact every individual who does that meditation in a similar way. Meditation requires active ongoing effort to focus attention. Each individual will have a unique experience with a meditation intervention.
The same meditation does not work equally well for everyone. The effectiveness of meditation depends on the predisposition and previous experiences of the individual. Meditation is a practice and a skill. Meditation is an active process whereby the participant is engaged in the process. The quality and extent of that engagement can have an effect on the outcomes of the meditation.
In a meditation session, an individual follows the instructions in the meditation, focuses their attention on an object and has an experience. The quality of the experience we have while meditating is influenced by the effectiveness of the meditation intervention, but also by factors such as (1) the state of our system at the time of doing the meditation (such as calm, distracted, focused, nervous, overwhelmed, centered, etc.), and (2) the level of skill at focusing our attention we have developed by practicing meditation over time. Other factors that determine the effectiveness of a given meditation include appropriateness of the meditation for the individual and appropriateness of the meditation for the symptom or condition. Also, if an individual has more of an interest in and intrinsic motivation to do a meditation, this will have an impact on the effect of the meditation.
9. Meditation Expertise
In meditation research, the meditation expertise of the individual or team who designed the meditation intervention should be described. If others delivered the intervention, their expertise should also be described. We suggest two categories to include when describing the expertise of the designer of a meditation intervention. The categories are: 1. Meditation approach/source (the body of knowledge the meditation originates from) and 2. Experience and practice (the meditation expert’s meditation experience -- # of years, training of the meditation expert, professional application of meditation).
For example, here are the two categories, used to describe the lead author’s meditation expertise.
-
Meditation approach/source: Yoga Therapy and Viniyoga of TKV Desikachar and classical Yoga as presented by The Yoga Sutras of Patanjali.
-
Experience and practice: Marcel is a certified Yoga Therapist (C-IAYT), has completed a 1000 hour Yoga Therapy training program, and a two year clinical internship. Marcel has been practicing Yoga Therapy as a clinical practitioner since 2010.
A challenge of studying meditation is that the researchers often do not have training or personal experience with meditation. Researchers plan the study, then hire a meditation expert to design and run the meditation intervention. Then the researcher analyzes the data and publishes the findings. The researcher is often not the meditation expert and the meditation expert is not the researcher. So we have situations where the researcher has limited understanding of meditation and the meditation expert has limited understanding of research and limited involvement in study design and interpretation. Involving a meditation subject matter expert as a consultant with research from start to finish helps to address this problem.
10. Conclusions
As researchers and meditation experts, we are always seeking to better understand meditation. Meditation is a general term that describes many different types of phenomena and interventions. The writing of this article arose out of a need for a framework that supports better understanding of research on meditation interventions. As researchers, we are trying to better understand the research on meditation. As meditation experts, we are trying to better understand meditation. The purpose of the meditation framework we have created is to support dialogue around meditation research and provide a common framework for making sense of meditation intervention research across different types of meditation and different applications of meditation.
There needs to be a way of understanding, comparing, and contrasting findings in research on meditation interventions. This article addresses a need and starts a dialogue for more rigor in describing and qualifying meditation intervention research. If researchers regularly apply our framework to describe all 7 components of a meditation intervention, individuals reading the research and future meta-analyses will be able to consider the potential influence of all of the components that characterize the intervention.
Published research comparing “types of meditation” could benefit from including our framework and then clarifying which element or elements they are comparing. For example, some studies have compared Mindfulness and Lovingkindness practices (two specific, common Buddhist meditations that are also part of Mindfulness Based Stress Reduction) [25,26,27]. Based on our framework, this comparison derives from both object and the experience of meditation.
Another study compared “three different meditation traditions (Vipassana, Himalayan Yoga and Isha Shoonya)” [28]. Based on our framework, this is a difference in the approach of the meditation. Still other studies define “types of meditation” based on how the meditation is delivered, such as whether it is led by an in person teacher or delivered via technology [29]. Based on our framework, this is a difference based on the delivery of the meditation. (Delivery is a component of experience).
We are certain that further development and application of a consistent and thorough framework like the one we propose will help researchers better understand, select, and describe meditation interventions as they design studies, and lead to a deeper and more comprehensive understanding of meditation as a health intervention. We also hope that the meditation framework will inform reporting and interpretation of research findings across diverse types of meditation and different approaches underlying meditation, and provide a strong foundation for cross-study comparisons.
We created the framework as a beginning point for understanding what is essential to describe about meditation interventions. This article is not a review of literature or a proposed new taxonomy of meditation. In developing the framework we asked ourselves, what are the essential elements to describe meditation as an intervention for health across different methods and techniques of meditation?
We offer the framework as a first step. These recommendations were developed by two authors whose meditation expertise is from the perspective of Viniyoga and Yoga Therapy [30,31,32]. It is our hope that researchers and meditation experts from different domains of meditation expertise will proof the framework we have offered by applying it. We encourage researchers, meditation experts, and healthcare professionals to consider the framework with their respective method of meditation. How is it useful? What needs to be added or modified to describe essential elements of their meditation interventions?
We hope that dialogue about and application of the meditation framework from different perspectives and practices will lead to refinements of the framework. Ultimately, the field of meditation intervention research would benefit from widespread use of this kind of framework as the basis for research reporting guidelines for meditation interventions.
Author Contributions
The authors contributed equally to conceptualizing and writing this concept paper.
Competing Interests
The authors have declared that no competing interests exist.
References
- Clarke T, Black L, Stussman B, Barnes P, Nahin R. Trends in the use of complementary health approaches among adults: United States, 2002–2012. Natl Health Stat Repo. 2015; 79: 1-15.
- Lutz A, Slagter HA, Dunne JD, Davidson RJ. Attention regulation and monitoring in meditation. Trends Cogn Sci. 2008; 12: 163-169. [CrossRef]
- Travis F, Shear J. Focused attention, open monitoring and automatic self-transcending: Categories to organize meditations from Vedic, Buddhist and Chinese traditions. Conscious Cogn. 2010; 19: 1110-1118. [CrossRef]
- Nash JD, Newberg A. Toward a unifying taxonomy and definition for meditation. Conscious Res. 2013; 4: 806.
- Khanna S, Greeson JM. A narrative review of yoga and mindfulness as complementary therapies for addiction. Complement Ther Med Kidlington. 2013; 21: 244-252. [CrossRef]
- Bossart C. Yoga Bodies, yoga minds: How Indian anatomies form the foundation of yoga for healing. Int J Yoga Ther. 2007; 17: 27-33.
- Bærentsen KB. Patanjali and neuroscientific research on meditation. Cognition. 2015; 6: 915.
- Monteiro LM, Musten RF, Compson J. Traditional and contemporary mindfulness: Finding the middle path in the tangle of concerns. Mindfulness. 2015; 6: 1-13. [CrossRef]
- Groessl EJ, Maiya M, Elwy AR, Riley KE, Sarkin AJ, Eisen SV, et al. The essential properties of yoga questionnaire: Development and methods. Int J Yoga Ther. 2015; 25: 51-59. [CrossRef]
- Travis F. Transcendental experiences during meditation practice. Ann N Y Acad Sci. 2014; 1307: 1-8. [CrossRef]
- Brown RP, Gerbarg PL. Sudarshan Kriya Yogic breathing in the treatment of stress, anxiety, and depression. Part II--clinical applications and guidelines. J Altern Complement Med N Y N. 2005; 11: 711-717. [CrossRef]
- Center for Mindfulness. History of MBSR [Internet]. Worcester: UMass Medical School; 2014 [2014 Dec 23]. Available from: http://www.umassmed.edu/cfm/stress-reduction/history-of-mbsr/
- Didonna F, editor. Clinical handbook of mindfulness. New York: Springer-Verlag; 2009. [CrossRef]
- Kabat-Zinn J. Some reflections on the origins of MBSR, skillful means, and the trouble with maps. Contemp Buddhism. 2011; 12: 281-306. [CrossRef]
- Sullivan MB, Erb M, Schmalzl L, Moonaz S, Noggle JT, Porges SW. Yoga therapy and polyvagal theory: The convergence of traditional wisdom and contemporary neuroscience for self-regulation and resilience [Internet]. Lausanne: Front Hum Neurosci; 2018 [2018 Apr 24]. Available from: https://www.frontiersin.org/articles/10.3389/fnhum.2018.00067/full
- Gard T, Noggle JJ, Park CL, Vago DR, Wilson A. Potential self-regulatory mechanisms of yoga for psychological health. Front Hum Neurosci. 2014; 8: 770. [CrossRef]
- Streeter CC, Gerbarg PL, Saper RB, Ciraulo DA, Brown RP. Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Med Hypotheses. 2012; 78: 571-579. [CrossRef]
- Farb N, Daubenmier J, Price CJ, Gard T, Kerr C, Dunn BD, et al. Interoception, contemplative practice, and health [Internet]. Lausanne: Front Psychol; 2015 [2015 Jun 19]. Available from: http://journal.frontiersin.org/article/10.3389/fpsyg.2015.00763/abstract
- Vago DR. Mapping modalities of self-awareness in mindfulness practice: a potential mechanism for clarifying habits of mind. Ann N Y Acad Sci. 2014; 1307: 28-42. [CrossRef]
- Davidson RJ, Dahl CJ. Outstanding challenges in scientific research on mindfulness and meditation. Perspect Psychol Sci. 2018; 13: 62-65. [CrossRef]
- Goleman D, Davidson R. The science of meditation: How to change your brain, mind and body. Penguin Books, Limited; 2017.
- Kaliman P, Alvarez-López MJ, Cosín-Tomás M, Rosenkranz MA, Lutz A, Davidson RJ. Rapid changes in histone deacetylases and inflammatory gene expression in expert meditators. Psychoneuroendocrinology. 2014; 40: 96-107. [CrossRef]
- Brefczynski-Lewis JA, Lutz A, Schaefer HS, Levinson DB, Davidson RJ. Neural correlates of attentional expertise in long-term meditation practitioners. Proc Natl Acad Sci. 2007; 104: 11483–11488. [CrossRef]
- Luders E, Toga AW, Lepore N, Gaser C. The underlying anatomical correlates of long-term meditation: Larger hippocampal and frontal volumes of gray matter. NeuroImage. 2009; 45: 672-678. [CrossRef]
- Zeng X, Chiu CPK, Wang R, Oei TPS, Leung FYK. The effect of loving-kindness meditation on positive emotions: a meta-analytic review [Internet]. Lausanne: Front Psychol; 2015 [2018 Jul 20]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4630307/
- Fredrickson BL, Boulton AJ, Firestine AM, Van Cappellen P, Algoe SB, Brantley MM, et al. Positive emotion correlates of meditation practice: A comparison of mindfulness meditation and loving-kindness meditation. Mindfulness. 2017; 8: 1623-1633. [CrossRef]
- Kok BE, Singer T. Phenomenological fingerprints of four meditations: Differential state changes in affect, mind-wandering, meta-cognition, and interoception before and after daily practice across 9 months of training. Mindfulness. 2017; 8: 218-231. [CrossRef]
- Braboszcz C, Cahn BR, Levy J, Fernandez M, Delorme A. Increased gamma brainwave amplitude compared to control in three different meditation traditions [Internet]. San Francisco: PLoS ONE; 2017 [2018 Jul 20]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5261734/
- Boxleitner G, Jolie S, Shaffer D, Pasacreta N, Bai M, McCorkle R. Comparison of two types of meditation on patients’ psychosocial responses during radiation therapy for head and neck cancer. J Altern Complement Med N Y N. 2017; 23: 355-361. [CrossRef]
- McCall T, Satish L, Tiwari S. History, philosophy, and practice of yoga therapy. Edinburgh: Handspring Publishing; 2016. page 17-30.
- Chandrasekaran N. Principles and practice of yoga therapy: A complete guide for learning and practice of yoga therapy. Chennai: VHP Publications; 2012.
-
International Association of Yoga Therapists. Educational standards for yoga therapists [Internet]. Little Rock: International Association of Yoga Therapists; 2016. Available from: http://c.ymcdn.com/sites/www.iayt.org/resource/resmgr/accreditationmaterials/ed_stds_sections/Educational
_Standards_2016-C.pdf.
