

Binary Model of the Dynamics of Active versus Passive Mindfulness in Managing Depression
Andrew J Hede * ![]()
- Professor Emeritus, University of the Sunshine Coast, Queensland, Australia
* Correspondence: Andrew Hede ![]()
Academic Editor: Sok Cheon Pak and Soo Liang Ooi
Special Issue: Health Benefits of Meditation
Received: July 27, 2018 | Accepted: December 20, 2018 | Published: December 24, 2018
OBM Integrative and Complementary Medicine 2018, Volume 3, Issue 4 doi: 10.21926/obm.icm.1804037
Recommended citation: Hede AJ. Binary Model of the Dynamics of Active versus Passive Mindfulness in Managing Depression. OBM Integrative and Complementary Medicine 2018; 3(4): 037; doi:10.21926/obm.icm.1804037.
© 2018 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
Background: Meditation has developed over many centuries within a diverse range of religious traditions including Middle-Eastern, Indian, and East-Asian. Of these, mindfulness meditation from the Buddhist (Indian) tradition, has been the most extensively adopted in the Western secular world primarily with applications in health and well-being as pioneered by Jon Kabat-Zinn.
Review: While originally developed to treat chronic pain and stress in the U.S., mindfulness training was later coupled with cognitive-behavioral therapy to treat depression in the U.K. and beyond. The present review of the literature confirms the effectiveness of mindfulness meditation in these medical applications. The various models of mindfulness that have been advanced are here reviewed and are shown to be generally based on an underlying unitary model of the human psyche. By contrast, the present model distinguishes between two modes of mindfulness, an active form and a passive form.
Theory: The foundations of these two modes of mindfulness are two of three posited types of self comprising the tripartite psyche, namely, the ‘intra-self’ (underpinning ‘active mindfulness’) and the ‘supra-self’ (underpinning ‘passive mindfulness’). The binary model of mindfulness advanced here shows how these two types of self can potentially form the basis of an effective two-stage approach to managing depression.
Application: By combining both cognitive decentering using active mindfulness and existential disidentification using passive mindfulness, individuals can learn to manage their cognitive dysfunction and distorted self-identity and thereby reduce the effects of depression in their lives. A design for an empirical study is provided to test the proposed model.
Graphical abstract

Keywords
History of mindfulness meditation; mindfulness training; models of mindfulness; binary model of self; cognitive decentering; existential disidentification; depression management
1. Introduction
It has long been recognized that depression is the most widespread mental illness impacting on human beings in modern times [1]. The World Health Organization (WHO) estimates that “depression is the leading cause of disability worldwide … Globally, more than 300 million people of all ages suffer from depression …” [2]. According to the American Psychiatric Association (APA): “Depression (major depressive disorder) is a common and serious medical illness that negatively affects how you feel, the way you think and how you act. Fortunately, it is also treatable. Depression causes feelings of sadness and/or a loss of interest in activities once enjoyed.” [3]. It is notable that the APA website as cited does not mention mindfulness despite the growing literature suggesting its effectiveness with depression and other conditions as will be shown.
The present paper aims to review the nature of mindfulness meditation and its development in Western medical applications (specifically, Mindfulness-Based Stress Reduction [MBSR] and Mindfulness-Based Cognitive Therapy [MBCT]), in particular, as they relate to depression. The paper also aims to review the various models that have been advanced for mindfulness efficacy by placing the proposed binary model of mindfulness in the context of other models in the established literature. After presenting the new binary model of mindfulness including an illustration of their distinct conceptual elements and also their key dynamic connections, the paper aims to provide a discussion of how this model compares with other models of mindfulness and the psyche. Finally, the paper aims to consider how the new binary model of mindfulness could be tested empirically with a field experiment based on the established MBCT program.
The predominant treatment for depression globally is currently antidepressant medication which has been increasing in usage throughout the modern era. Total antidepressant use in the U.S., for example, was reported in 2011 by the National Center for Health Statistics as having increased by 400% over the previous two decades such that 11% of Americans are currently estimated to be using antidepressants [4]. This is despite the fact that mindfulness meditation has been verified in many studies and reported in top medical journals as an effective alternative to medication for the treatment of depression [5,6]. While mindfulness training was introduced in the West initially to assist people in managing stress [7,8,9], this form of meditation has since been expanded in its application to a range of mental illnesses [10] including depression [11,12], anxiety [13,14] and bipolar disorder [15,16]. In addition, there is some expirical evidence that mindfulness meditation may play a positive role in ameliorating some non-neurological aspects of various neurological conditions such as chronic pain [17,18], Parkinson’s disease [19,20], dementia [21], epilepsy [22] and multiple sclerosis [23,24]. However, it is not yet known how mindfulness might alter the course, prognosis, or underlying pathophysiology of such neurological conditions [Anonymous reviewer, Email, December, 2018].
2. Review of Mindfulness Meditation
Meditation, as it is currently practiced across both the spiritual and secular worlds, originated with religious observances in India dating to before recorded history. Contemporary scholars have observed that there are strong similarities among the various religious traditions in their meditation practices including: those of Biblical origin in the Middle-East (viz., in chronological order – Judaism, Christianity and Islam) [25]; traditions of Indian origin (e.g., Hinduism, Buddhism, Jainism and Sikhism) [26,27]; and also those of East-Asian origin (e.g., Daoism, Confucianism and Shintoism) [27]. Within each of these traditions there have arisen variations in meditation practices that are relevant today. To elaborate on one pertinent example, the main active Buddhist meditation tradition contains two distinct sub-traditions which spread over many years as part of the cultural growth of a number of Indian and Asian countries. The first of these sub-traditions is Mahayana meditation (including Zen) which developed in China, Korea, Japan, Tibet and Vietnam [28]. The second Buddhist sub-tradition is Theravada meditation which spread mainly in Sri Lanka, Thailand, Myanmar, Laos and Cambodia [28]. These two meditation practices have spread widely including to Western countries. For example, the Vietnamese Zen Buddhist monk, Thich Nhat Hanh, has been successful in promoting a blend of both Mahayana and Theravada meditation practices in the English-speaking world, principally in America [29].
Observances in meditation practice have not always been consistent within the various traditions over the centuries. An informative example is a type of meditation which was developed in the 4th Century CE by the Christian hermits of the Mediterranean. This meditation practice was based on focusing attention on the unceasing repetition of a short exhortation [30]. Such a prayerful exclamation functions in this form of meditation as a focal point for the ‘busy mind’ somewhat like the mantra in Hindu practice and related forms of meditation [31]. Following the so-called ‘East-West Schism’ in the Christian Church (from 1054 CE) [32], this meditation practice continued to be promulgated throughout the Eastern (Orthodox) Church through to the present day [33], but was largely ignored for nearly a millennium within the Western (Roman) Church [34]. There was a revival of this ‘desert meditation’ tradition late last century led by Benedictine monk, John Main. It is significant that he was initially trained in Hindu meditation practice and that he promoted what he called ‘Christian Meditation’ with the personal support of his friend the Dalai Lama, world leader of Buddhism [35]. It should not be surprising that Christian, Buddhist and Hindu meditation influences all converged in this contemporary meditation movement which is thriving in the 21st Century. It would appear that meditation practices have been at the core of human experience across the ages linking diverse religions and cultures. We can only speculate about the possible health benefits ancient peoples might have gained incidentally from their spiritual practice of meditation thousands of years ago.
Of the many Buddhist meditation traditions and practices, the one that has attracted most attention and acceptance in the Western world is ‘mindfulness’ (called ‘sati’ in the Pali language as used in the Theravada tradition and called ‘smrti’ in the Sanskrit language as used in the Mahayana tradition) [36]. This is the main Buddhist form of meditation and can be traced to the original Buddha (Siddhartha Gautama, c.500 BCE). The English translation of ‘sati’ as ‘mindfulness’ is credited to Rhys Davids in 1881 [37]. From the earliest times of Buddhism, distinctions were drawn between different forms of meditation, namely, mindfulness (sati), concentration meditation (samadhi), supramundane powers (abhijñā), tranquillity meditation (samatha) and insight meditation (vipassanā) [37].
2.1 Spread of Mindfulness Meditation in the West
Mindfulness meditation was already being taught in the U.S. as part of various international Buddhist education programs from the mid-20th Century [38,39,40,41]. But it was not until Jon Kabat-Zinn established the Centre for Mindfulness at the University of Massachusetts Medical School in 1979 that this approach engaged reputable institutions in the West [7,8,9]. This was evidently due to the program’s scholarly reputation, its effective marketing and its high participant satisfaction. A major factor in the acceptance of mindfulness meditation in America was that it was promoted with few religious trappings [42].
A recent popular article has claimed that Rhys Davids’ original translation of ‘mindfulness’ was not entirely accurate, suggesting to the contrary that ‘mindfulness’ really means ‘memory of the present’ [43]. However, a more authoritative Buddhist source asserts that ‘mindfulness’ as traced to its original roots would best be characterized as ‘lucid awareness’ or more precisely “the element of watchfulness, the lucid awareness of each event that presents itself on the successive occasions of experience” [44]. Kabat-Zinn promoted the following definition which has been widely adopted: "Mindfulness means paying attention in a particular way: on purpose, in the present moment, and nonjudgmentally." [8]. The author can vouch for these three simple defining features being very effective in teaching mindfulness to executives in university courses. Thus, with its accessibility in practice, its hints of exoticism and its lack of emphasis on religion, mindfulness has proved very marketable to a Western secular audience especially when used for ‘respectable’ university medical purposes.
As well as establishing an educational base for mindfulness in the U.S., the University of Massachusetts Center for Mindfulness quickly became the springboard for mindfulness training in other English-speaking countries especially in the U.K. where leading researchers applied it to treating mental illness principally relapses in depression [45,46]. In the almost 40 years since the original centre was launched, the Centre’s website indicates that more than 24,000 people have completed at one or other of their courses including the original 8-week Mindfulness-Based Stress Reduction (MBSR) course and more recently, various online mindfulness courses [47]. Significantly, many of these course alumni would have gone on to conduct their own mindfulness courses in their own country thereby continually spreading this approach. For example, the website of Dr Russ Harris in Australia reports that the 30,000 individuals who have undertaken short courses in Acceptance and Commitment Therapy (incorporating mindfulness) since 2005, have almost all been health professionals [48]. Further, there appears to be a clear trend of incorporating mindfulness as a mainstream topic into university psychology courses around the world and this will presumably ensure the ever-growing adoption of mindfulness in future clinical psychology practice [49].
However, considering this high rate of adoption of mindfulness in the secular world, the question arises as to how this compares with the original spiritual meditation practice handed down within Buddhism. According to one learned source, some modern Buddhists are concerned that modern mindfulness is becoming alienated from the traditional Buddhist approach [37]. Not surprisingly, many medical and psychological practitioners endeavour to teach mindfulness divorced from spiritual meditation as alluded to previously. Indeed, an influential article titled ‘Mindfulness Without Meditation’ asserts: “’Mindfulness’ can be defined in a variety of different ways, but they all basically come down to this: paying attention with flexibility, openness, and curiosity.” [50].
As an indicator of Western acceptance of mindfulness, it is worth considering that the American Mindfulness Research Association (AMRA) has been collating all the scholarly journal articles on mindfulness which have been published worldwide since 1980. Their latest official records [51] yield the following figures up to 2017: in the 20 years between 1980 and 2000, there were a total of only 58 publications on mindfulness; in the decade between 2001 and 2010, there were a further 578 publications; and between 2011 and 2017 there were 3,149 mindfulness publications. The cumulative total to 2017 was 3,785 publications which is currently increasing at almost 700 publications per year.
In his recent recollections long after establishing the Centre for Mindfulness, Kabat-Zinn commented that in his first book on mindfulness published in 1990 [9], his intention was to “embody to whatever degree possible the dharma essence of the Buddha’s teachings put into action and made accessible to mainstream Americans facing stress, pain, and illness.” [7]. Kabat-Zinn further elaborated on his use of the Buddhist concept of ‘dharma’ in the following words: “The intention and approach behind MBSR [Mindfulness-Based Stress Reduction] were never meant to exploit, fragment, or decontextualize the dharma, but rather to recontextualize it within the frameworks of science, medicine (including psychiatry and psychology), and healthcare so that it would be maximally useful to people who could not hear it or enter into it through the more traditional dharma gates, whether they were doctors or medical patients, hospital administrators, or insurance companies.” [7].
We see then that Kabat-Zinn openly employed the spiritual/religious language of Buddhism in launching mindfulness in the U.S. (particularly in promoting ‘dharma’ as illustrated in the quotations above). Thus, Kabat-Zinn found a way of promoting Buddhism in a secular Western medical framework almost four decades ago, without diluting its essential Eastern message and without alienating potential Western converts to mindfulness meditation. In the words of an American radio interviewer, Kabat-Zinn was promoting the concept of “Buddhist meditation without the Buddhism”. In a broadcast interview in 2010, Kabat-Zinn succinctly summarized his own position in these terms: “You understand that I myself am not a Buddhist, right? I don’t see what I do as Buddhism so much as I see it as Dharma expressing itself in the world in its Universal-Dharma-way” [52].
3. Mindfulness Meditation Applications in Health & Well-Being
3.1 Mindfulness-Based Stress Reduction (MBSR)
The MBSR (Mindfulness-Based Stress Reduction) training programs dating from the early 1980s in the U.S., were initially designed to treat patients with chronic pain and typically comprised eight weeks of group instruction weekly, plus an all-day retreat, coupled with daily mindfulness practice individually [53]. This 8-week blueprint became the basic formula for medical mindfulness training that has persisted in the West till today. A concise summary of the underlying foundation of medical training in mindfulness within and beyond the U.S., was provided in a recent article by Dutch researchers as follows: “The MBSR- and MBCT protocol comprises both focused attention, open monitoring, and breathing meditation but without the transcendental atmosphere of traditional meditative practice.” [54].
The structure of the original MBSR training course (that was adapted for MBCT) is presented on the website for Kabat-Zinn’s first book [9], and comprises:
Eight weekly classes, 2 1/2 hours each (totalling 31 hours direct instruction);
One All-Day class on a Saturday or Sunday [7.5 hours], between classes 6 and 7;
Daily home practice assignments for 45-60 minutes each day;
Guided instruction in mindfulness meditation practices;
Gentle stretching and mindful yoga;
Group dialogue and discussions aimed at enhancing awareness in everyday life;
Systematic instruction in formal MBSR meditation practices, with opportunity to check in with teachers;
Daily home assignments;
Downloadable home practice audio files (or CDs) and a home practice workbook” [55].
Before examining MBCT and its application in the treatment of depression, it is worth briefly reviewing the key studies assessing the original medical mindfulness program, MBSR. Specifically, we will review three meta-analyses each of which assessed the results of multiple studies [10,56,57]. First, a review by Grossman et al. in 2004 identified 64 relevant studies of MBSR but found that only 20 studies covering 1,605 subjects met their stringent criteria for inclusion. Their results indicated that both controlled and uncontrolled studies had comparable effect sizes (i.e., Cohen’s d values ≈ 0.5). Although warning that their results are not definitive because of deficiencies in the rigour of the 20 studies included, the investigators concluded that their meta-analysis showed that “Mindfulness training may be an intervention with potential for helping many to learn to deal with chronic disease and stress.” [10].
The second meta-analysis worth considering here is that conducted in 2009 on 10 studies of MBSR that qualified out of 150 relevant publications identified [56]. According to the researchers, these studies were of ‘mainly low quality’ because of deficiencies in their control conditions. Across these 10 studies the pre-post comparison effects of mindfulness on stress levels as measured by the Cohen’s d statistic, were in the range between 0.5 and 1.00 which is accepted as statistically significant. This study also included a specific comparison of MBSR with standard relaxation training and found that the two behavioral conditions were equally effective in reducing stress. Nevertheless, this study is limited in its outcomes because of the lack of precision in the controls of its component studies which point to the need for further research. The third and most recent meta-analytic study, dating from 2015, initially examined 400 published articles and ultimately selected 29 studies of MBSR interventions which met their rigorous inclusion criteria. Note that these studies included a total of 2,668 individual subjects [57]. Effect sizes were measured using the statistic Hedge’s g with individual studies showing effect sizes around 0.5 which is considered moderately large. The researchers note that despite limitations arising from various methodological issues, this meta-analysis is consistent with several previous ones they had published which provide evidence for the effectiveness of MBSR interventions [57]. Again, however, these researchers stress that further research is needed.
A variant on the above meta-analysis was conducted by researchers who investigated different systematic reviews of studies which employed randomized control trials (RCTs) to assess the effectiveness of mindfulness interventions (viz., MBSR and MBCT) [58]. They initially identified 187 relevant reviews of which 23 qualified for inclusion and yielded 115 different RCTs covering 8,683 patients suffering various conditions, physical and psychological. This research is distinctive for its methodological rigour in that all of the studies selected used randomization as well as a control group. By making comparisons with suitable control groups, the researchers found there were significant improvements due to mindfulness in a number of conditions, namely, stress, depression, anxiety, quality of life, and general physical functioning [58]. Clearly, this broad study shows there is considerable evidence for the effectiveness of MBSR and MBCT across a range of health conditions, though there is some null evidence in the literature as well.
3.2 Mindfulness-Based Cognitive Therapy (MBCT)
Mindfulness-Based Cognitive Therapy (MBCT) can be considered a blending of mindfulness training from MBSR together with the long-established approach to treating mental illness known as cognitive-behavioral therapy (CBT) [59]. The MBCT course in general use is directly comparable to the 8-week MBSR course (outlined above). According to the official MBCT website, the course “allows participants to become aware of how conditioned patterns of mind and mood can trigger depression relapse and sustain current symptoms of depression. Through the practice of mindful awareness, they develop the capacity to mindfully disengage from distressing moods and negative thoughts.” [60]. The origins and development of CBT are comprehensively reviewed in Dobson’s definitive handbook [61]. The precursors to the emergence of MBCT comprised studies in the 1980s such as a study that compared the effectiveness of CBT with that of relaxation training (similar to mindfulness) [62]. The subjects in this case were 30 moderately depressed adolescents as assessed on the validated instrument, the Beck Depression Inventory (BDI) [63]. Subjects were randomly assigned to either the CBT or relaxation treatment groups or else to a ‘wait-list’ as a standard though not ideal (as compared with active) control. Subjects who underwent either form of treatment experienced a lowering of their depression from an average of moderate to non-depressed and maintained this improved level at a follow-up assessment. The results indicated that after five weeks’ treatment, there was no significant difference between the CBT and relaxation conditions thereby providing a basis for a combined treatment approach [62].
3.3 Research on MBCT and Depression
After the U.S. Mindfulness Centre had been operating for 20 years training people via the 8-week MBSR course as outlined above, investigators in the U.K. combined this mindfulness program with the already established cognitive-behavioral therapy (CBT) in the treatment of depression [45,46]. In what is generally accepted as the inaugural research study of MBCT by Teasdale and colleagues in 2000, 145 individuals in remission or recovery from major depression were randomly allocated to either a group undergoing an 8-week course based on MBSR or to a treatment-as-usual (TAU) group [46]. When tested after one year, 40% of those in the MBCT group were found to have suffered depressive relapse whereas 60% of the TAU group experienced depressive relapse, a significant difference. These results have been replicated in subsequent studies [11,64,65,66].
A further example of the extensive research on this moderately new method (MBCT) is a major study published in 2016 in which researchers initially located 286 studies of MBCT in the relevant databases (n=5), and then identified 41 of these articles for detailed evaluation and finally selected 16 studies as fully qualifying for analysis [11]. The main outcome measures were possible differences in 1-year relapse rates and possible pre-post differences in scores on the Beck Depression Inventory (BDI). The 16 selected studies were subjected to detailed analysis and were reported in depth in the published article. An important finding of this meta-analysis was that the combination of MBCT plus gradual withdrawal from anti-depressant medication did not significantly lower depression relapse rates [11]. Although not emphasised by the researchers, the results of this study showed that in treating depression, there are complex interactions among the so-called ‘active ingredients’ of MBCT and other medical and non-medical factors in patients’ lives [11].
Another relatively recent study examined research which investigated individuals who had undergone non-pharmacological treatment after they had recovered from depression. In this meta-analytic study, a search of the major databases revealed 29 eligible published interventions comprising 2,742 individuals [65]. The results were compared after 12 months of treatment (viz., either cognitive-behavioral therapy [CBT], mindfulness-based cognitive therapy (MBCT) or interpersonal psychotherapy (IPT). The findings indicated that these three primary treatments were associated with a 22% reduction in depressive relapse as compared with individuals in the control conditions. After 24 months these effects were maintained for treatments involving cognitive-behavioural therapy but not for that with IPT alone. The researchers conclude that interventions using psychological treatments may assist in the recovery of depression sufferers’ experience because of pharmaceutical treatment or acute psychological therapy [65].
A recent meta-analysis updated a previous study by screening 2,555 new studies of which only 9 studies met all the inclusion criteria thereby yielding 1,258 eligible patients [66]. The meta-analytic results indicated that those patients who had undergone MBCT were significantly less likely to experience a depressive relapse within 60-weeks of treatment in comparison with patients who did not undergo MBCT. In addition, the results showed a reduced risk of depressive relapse with MBCT as compared with active treatments within a 60-week follow-up. The researchers concluded that MBCT can be efficacious in preventing relapse for those suffering recurrent depression [66]. This study was included in a review by Oxford University’s Mindfulness Centre published on their website in 2016 in which they asserted: “Consistent with the findings of previous meta-analyses, our work indicates that MBCT provides clear benefit over control conditions (comprising usual care in some studies and active controls in others), through reducing rates of relapse to depression over 60 weeks follow-up.” [67]. The Oxford University review concluded that: “The results of this meta-analysis are promising and suggest that MBCT can provide a viable relapse prevention intervention for people with a history of recurrent depression.”
4. Review of Models of Mindfulness Efficacy
Having established that mindfulness meditation can be effective in a number of important areas of mental health, it’s appropriate to consider what are the theoretical models which explain the underlying mechanisms of mindfulness, a topic that has been subjected to extensive analysis over the past two decades. One of the earliest reviews of mindfulness models was that by Baer in an influential paper that also reviewed the meta-analytic studies that had been published at the time (2003) [68]. From the empirical viewpoint, this investigation concluded that despite many methodological flaws, the available research indicated that mindfulness-based interventions can be effective in treating a number of disorders. From the conceptual viewpoint, Baer also showed that there were a variety of theoretical models (explicit and implicit) which aimed to explain the efficacy mechanisms of mindfulness in health applications [68].
A relatively early attempt to conceptualize the efficacy mechanisms involved in mindfulness interventions, was an article by Bishop and associates which presented a two-component model to provide an operational definition of mindfulness [69]. As the researchers described their model: the first component is that of self-regulation of attention based on immediate experience which allows for increased recognition of mental events in the present moment. The second component refers to an individual’s ability to orient themselves toward their experience in the present moment, an orientation that involves curiosity, openness and acceptance [69]. While Bishop’s model posits two operational components in mindfulness, it is worth noting that this differs from the binary model advanced in this paper which is based on there being two mindfulness processes (active versus passive) underpinned by two structural elements (‘intra-self’ versus ‘supra-self’) (see Figure 1).
Some of the important conceptual models of mindfulness are associated with the various instruments developed to measure mindfulness competencies in individuals. In other words, the dimensions or factors of the instrument correspond with the constructs in the model. For example, the empirically validated ‘Five Facet Mindfulness Questionnaire’ advanced by Baer and colleagues, is designed to assess five component skills yielding a five-factor conceptual model of mindfulness (viz., “observing, describing, acting with awareness, nonjudging of inner experience, and nonreactivity to inner experience” [70]. Another example from those available is a conceptual model that posits two basic components of mindfulness, specifically, 1) present-moment awareness, and 2) non-judgmental acceptance of thoughts and emotions. These two components are proposed to operate iteratively so as to promote executive control which leads to an improvement in the regulation of emotion [71]. A comprehensive conceptual review worth noting in this context is one by Brown and associates that compared the mechanisms of mindfulness proposed in ancient Buddhist versus contemporary secular scholarly sources [72]. They review the mindfulness mechanism of attention and the role it plays in the regulation of both physical and psychological health. In addition, they review the main theories of behavioral regulation (e.g., self-control) and evaluate the importance of paying attention here and now, a key mindfulness practice.
A recent pivotal paper which investigated six different models of the efficacy mechanisms involved in mindfulness-based interventions (MBI) [73]. This study analysed 20 methodologically-acceptable published articles (out of 169 relevant full-text publications) relating to MBSR (mindfulness-based stress reduction) and MBCT (mindfulness-based cognitive therapy). Using two-stage structural equation modelling the research identified four main mechanisms that proved effective, namely: mindfulness (present moment awareness with non-judgmental acceptance), repetitive negative thinking (comprising rumination about the past and worrying about the future), self-compassion (including self-acceptance) and cognitive and emotional reactivity (which entails stress triggering negative thinking and emotional behaviors). The researchers concluded that their study indicated the evidence for cognitive and emotional reactivity was stronger than the other mechanisms investigated [73].
A somewhat different model of mindfulness emphasizes the role of ‘positive reappraisal’ of conditions which pose either a stressor or a threat to an individual [74]. The function of positive reappraisal is to operate as an active coping strategy which re-evaluates the stressor and alters how it is experienced. This model of mindfulness posits that in order to obtain a state of positive reappraisal, an individual has to retreat from their initial appraisal of an event into a momentary state of metacognitive awareness that discards the original semantic evaluations one made and replaces them with positive evaluations [74]. Thus, positive reappraisal is the central mechanism in this so called ‘mindful coping model’ which is posited to result from the instrumentation of mindfulness. This model, while primarily focusing on the effect of mindfulness on stressors, can be extended to explain the dynamics of depression.
A recent systematic review by van der Velden and associates focused specifically on the mechanisms in MBCT which produce change in patients suffering major depressive disorder [75]. The researchers initially identified 476 relevant studies of which 23 were eligible for analysis. Of these, 12 studies indicated that changes in mindfulness, rumination, worry compassion or meta-awareness were associated with the treatment effect of MBCT. In addition, there were a number of other mechanisms (including alterations in attention and emotional reactivity) that were identified as possibly playing a role in the efficacy of MBCT subject to further research. Another recent model of the mechanisms of mindfulness has been called ‘monitor and acceptance theory’ (MAT) which succinctly describes the two constructs on which it is based [75]. This theoretical approach adopts the widely accepted definition of mindfulness as its core (viz., present moment attention plus non-judgmental acceptance), specifically, attention monitoring and acceptance [76]. According to MAT theory, the initial efficacy mechanism in mindfulness practice should be an increased capacity for attention monitoring. Such a capacity should enable an individual to be more aware of affective information and if they are operating alone, this skill should reduce their negative experiences and increase their positive experiences. Note that the MAT model is comparable to that offered by Bishop et al. as considered above, in that both are based on two-components (attention and acceptance) [69].
A significant review published recently, systematically examined the various ‘mechanisms of action’ that have been advanced to explain the efficacy of the main mindfulness-based interventions, (MBCT and MBSR), while adopting the definition of ‘mechanism’ as a process that can bring about change in a patient’s physical or psychological condition [77]. The researchers scanned 7 major databases and initially identified 3,290 studies of which 3,234 were removed for various reasons leaving 41 possible studies for further consideration. After further exclusions, they finally selected 4 studies of mindfulness treatments for combined physical and psychological conditions and a further 14 studies of various psychological conditions. The researchers commented on the general lack of methodological rigour in the studies analyzed but concluded that overall there was clear evidence for the efficacy of mindfulness interventions. However, regarding the mindfulness mechanisms at work in treating depression, they found that of the 14 studies of psychological conditions, most related to depression and that the key mechanisms in addition to mindfulness were “rumination, worry and self-compassion” as well as “attention and emotional reactivity” [77]. Again, the authors state that further research is needed to clarify the dynamics involved.
Finally, in a novel study published this year, Britton and colleagues observed that mindfulness-based interventions (viz., MBSR and MBCT) employ two distinct practices, namely, focused attention (FA) and open monitoring (OM) [78]. These two meditation practices were identified previously by Lutz and associates [79] as being central to mindfulness-based programs. Britton et al. assert that FA involves four interrelated skills: “1) sustaining attention on a chosen object; 2) identifying distractions without destabilizing the intended forms; 3) disengaging from a distracting object without further involvement and 4) redirecting focus promptly to the chosen object.” [78]. The second type of meditation, OM (open monitoring), is claimed to involve the cultivation of non-reactive awareness of the automatic cognitive and emotional responses one has to the continual barrage of stimuli they receive.
Using samples matched on relevant variables, this research compared a mindfulness-based intervention that was primarily based on focused attention (FA) with one based on open monitoring (OM) and also using the standard MBCT program as a third treatment functioning as an active control group [78]. After 506 potential participants were initially assessed, a total of 104 subjects were selected and randomly assigned to one of the three treatment groups. Each group underwent approximately 3 hrs/week of group instruction in the relevant meditation practice plus comparable times in directed daily meditation practice and reading. With a number of drop-outs from the 8-weeks training, 96 subjects were finally judged eligible for analysis spread roughly equally across the three treatment groups. At the end of their respective 8-week course, each subject completed 7 different self-report instruments including one scale, the Therapeutic Factors Inventory, comprising 99 items. The results indicated that the three treatment groups (FA, OM and MBCT) differed in the skill levels subjects acquired on the various instruments [79]. Essentially, this research demonstrated that the two primary components of mindfulness practice can be differentially enhanced by training directed at either focused attention or open monitoring. In the present context, this means that a two-component model of mindfulness (FA versus OM) can have practical application.
The above overview of models of mindfulness which is based on a diverse selection from the many published conceptualizations of mindfulness efficacy, shows that there has been a variety of mechanisms postulated to explain how mindfulness can produce beneficial physical and psychological health effects. Coupled with the extensive empirical evidence reviewed previously, there is considerable evidence for the effectiveness of mindfulness interventions in the treatment of depression and other mental conditions. One feature that all the models share, albeit without specifying the fact, is that they postulate that the human psyche is unitary and, consequently, that mindfulness is a unitary process. The binary model of mindfulness proposed in this paper is based on the concept of two distinct processes (‘active mindfulness’ versus ‘passive mindfulness’) occurring in a tripartite human psyche comprising three distinct selves as described (viz., the ‘sub-selves’, the ‘intra-self’ and the ‘supra-self’). The present model (see Figure 1) is developed from that proposed some years ago in relation to executive stress [80] and more recently applied to environmental noise stress [81].
Despite the considerable evidence for the efficacy of mindfulness as reviewed above, there is a new literature that is critical of mindfulness and cautions scientists, the public and the media to “mind the hype” [82]. Van Dam and associates recently published a detailed critique with the objective of addressing the “Misinformation and poor methodology associated with past studies of mindfulness [which] may lead public consumers to be harmed, misled and disappointed” [82]. These critics place particular emphasis on the difficulties in defining mindfulness as well as the alleged deficiencies in the methodology of mindfulness research. Regarding the definition of mindfulness, there is certainly a need for an international standard classificatory system to ensure that therapeutic practices and comparative research studies are consistent. As well as the issue of defining mindfulness, the van Dam group questions the construct validity of mindfulness and also the problems of operationalizing and measuring mindfulness especially via self-report questionnaires. In addition, they advocate a new prescriptive protocol for therapeutic interventions involving mindfulness.
A reply to the above critics was recently presented by Davidson and Dahl [83] who reported that they accepted van Dam’s main points, but that there are a number of issues regarding future mindfulness research that need to be considered. The main issues Davidson and Dahl raise include the fact that mindfulness is not the only research area to face problematic methodological concerns especially the use of self-report measures [83]. Further, as has been shown in the present paper, the term mindfulness has a long history and has come to be applied to a diversity of meditation practices. Both groups of evaluators warn of the tendency for previous research studies to mismatch diverse meditation training under the single rubric of mindfulness [82,83]. I would observe that such an approach is likely to confound ‘what causes what’ when accounting for research results. The van Dam group continued the debate by offering a rejoinder to Davidson and Dahl [83,84]. While conceding that methodological issues are not unique to mindfulness research, van Dam and colleagues stress that they are still of great importance even allowing for the relative youth of the discipline [84]. It is worth noting that mindfulness applications in health and wellbeing can be traced only four decades to around 1980 (for MBSR [17]) and two decades to 2000 (for MBCT [46]). The key lesson from the recent van Dam debate would seem to be that mindfulness research over the next 20 years needs to focus on systematically assessing the efficacy of the various relevant mindfulness practices and also to apply more standardized and more objective measures with less reliance on self-report.
5. Proposed Binary Model of Mindfulness
The current model draws on the vast literature reviewed above, to propose that mindfulness can have a beneficial effect on depression firstly, by assisting patients in disengaging from their negative thoughts and secondly, by helping them disidentify with the self that sustains their depressive existence. The mechanisms involved in mindfulness meditation are posited to be as indicated in the literature, namely, the active process of focused attention and also open monitoring which is, as will be shown, not entirely passive [68,77,78] in contrast to the present (active versus passive) model. The present binary model of mindfulness proposes that the human psyche comprises a number of distinct mental components which give rise to two modes of mindfulness to be considered later. The first mental component, the ‘sub-selves’, are the basic operating elements of one’s psyche; they dominate an individual’s waking consciousness and comprise the ever-present ‘voices in one‘s head’ experienced by every person capable of thought. The ‘sub-selves’, ‘intra-self’ and’ supra-self’ are not ontologically-distinct entities within the human psyche and are in that respect parallel to Freud’s model of the psyche comprising the id, ego and superego which are posited to be emergent entities [85]. Rather, the present tripartite selves are theorized as constructs which emerge from distinct functions of the psyche. For example, the ‘sub-selves’ emerge from the repeated patterns in the stream of ‘mindchatter’ that continually occupies our consciousness [80,81].
In the case of depression, it is here posited that it is the sub-selves which feed one’s mind non-stop with the negative thoughts that initially create the state of depression and subsequently serve to maintain its hold over the individual’s life. Fortunately, however, it is the sub-selves which respond to cognitive-based interventions in the treatment of depression [62,63]. It has been found to be beneficial in managing our sub-selves to label them with names which describe the typical thoughts that each produces – Voice Dialogue is a well-established therapeutic technique for helping individuals understand the various components of their own psyche including their various sub-selves [86,87]. For example, while each person has their own set of sub-selves approximately 4-6 of which are typically operative at any one time and which contribute either positively and negatively to their ‘mindchatter’, most individuals share a sub-self that can be labelled ‘The Miserable’ (‘Poor Me’) as well as another we can label ‘The Critic’ (‘You’re Pathetic’) [86]. It is here asserted that these are the two sub-selves that are the primary sources of constant depressive thoughts such as: “You are hopeless; your life is a failure; you’re a loser; why don’t you just give up! ... etc.” (viz., ‘The Critic’ sub-self), and also: “Depressed is me; I’m so sad; I am worthless; my life is meaningless; no-one cares about me; there’s no hope – I might as well opt out of this life … etc.” (viz., ‘The Miserable’ sub-self). Cognitive therapy, with or without mindfulness, aims to help patients firstly observe their negative thoughts, and then to recognize such thoughts as erroneous, and eventually to detach from these thoughts as not being their own self [45].
Mindfulness teaches individuals to reach such detachment via open self-observation during meditation [78]. Unless an individual can detach themselves from such negative thoughts, they are likely to identify their very being with such thoughts and thereby to become identified with their own negative thoughts. It’s as though they say in a variation of Descartes: “I think; therefore, I am… my thoughts”. As cognitive therapy has revealed over several decades, depressive individuals tend to believe their own thoughts, including their illogical negative thoughts, and to regard them as indubitable ‘inner truths’. The ever-present ‘mindchatter’ they experience, especially those ongoing streams of negative thoughts from their sub-selves that criticize and undermine everything they are and do, reinforces their sense of hopelessness. Such individuals come to identify with their own depressive thinking without realizing that their true self is able to observe their mind and that, consequently, they are a being beyond their mind and, therefore, they are not subservient to the relentless ‘mindchatter’ of their mind, specifically, their negative but persuasive sub-selves. Addressing this erroneous thinking is the key strategy proposed by the present binary model in managing depression. The other key strategy is existential disidentification to be considered later.
As well as the ‘sub-selves’, the human psyche comprises the structural component of the ‘intra-self’ (intra = ‘within’ …the mind and among the sub-selves). The intra-self functions as each person’s ‘managing ego’ or in an alternative framework, their ‘aware ego’ [86,88]. This component of the psyche is responsible for managing the challenges a person faces each day. The intra-self actively operates within the realm of the ‘mindchatter’ of the sub-selves and provides the individual with constructive feedback contrary to the negativity of ‘The Critic’ and ‘The Vulnerable’ [86]. The intra-self is an active component of one’s psyche which plays two roles under the main form of mindfulness, namely, ‘active mindfulness’. These active roles are: 1) to manage the continuous focussing of attention in the present moment, and 2) to maintain an open state of active monitoring of their own mind without any judgement, commentary or intervention [78]. This active form of mindfulness is generally regarded as the only type of mindfulness in modern psychology and medicine, that is, as the active but neutral form of monitoring the processes of one’s mind [67,71].
The third and final structural component of the human psyche is the ‘supra-self’ (supra = ‘above’ …the mind). The supra-self is also aptly described as the ‘inner observer’ or ‘observing self’ [89 and that is how it plays a critical role in the mindfulness-based management of depression (as will be shown later). The supra-self is one’s ‘higher self’ which functions above the mind, meaning that it is completely neutral and totally detached from the ‘mindchatter’ of the sub-selves including those that feed depressive thinking. However, most people identify with their mind such that they regard their mind as their ‘true self’. Moreover, they are completely unaware of their supra-self, much less of its ability to detach from the reactivity and the frequent chaos of their sub-selves and their ‘mindchatter’. From all that is known from 2,500 years of scholarly human psychology, originating with the teachings of the Buddha and now widely accepted in Western psychology and medicine, the mind and its vicissitudes can be well managed through mindfulness [60,67].
Significantly, the supra-self is almost invariably either unrecognized or disregarded not only by individuals most in need, but also by entire disciplines within psychology and medicine. It is notable that mindfulness meditation is currently regarded in psychology and medicine as a legitimate and effective intervention in a range of illness conditions including depression However, there is virtually no recognition in the literature of a higher form of self which operates passively above the cognitive domain of the mind and which can foster true detachment from the negative thought processes which feed depression. As far as is known, the supra-self can be engaged only by ‘stillness meditation’ which enables one’s higher self to observe with passive detachment. Repeated practice of stillness meditation eventually leads an individual to disidentify their existence from their depressive self. This results from the following simple but compelling logic: “If I can repeatedly observe my mind and its constant chatter as other, then my true self must exist separately from my mind”. Disidentification from one’s mental illness can free a depressed individual from the heavy burden of their unceasing negative thoughts and enable them to experience increased self-affirmation [90].Thus, it is here proposed that the human psyche has three structural components: 1) the ‘sub-selves’ responsible for one’s constant ‘mindchatter’, 2) the ‘intra-self’ which performs the function of one’s managing ego, and 3) the ‘supra-self’ which is one’s higher self and which operates above mind as one’s inner observer. Both the intra-self and the supra-self participate in mindfulness activities, the former by performing ‘active mindfulness’ typically involving both focused attention and open monitoring, and the latter engaging in ‘passive mindfulness’ which is entered via stillness meditation. In addition to the structure of the psyche, the present binary model of mindfulness hypothesizes about the way the psyche functions in managing depression (see Figure 1).
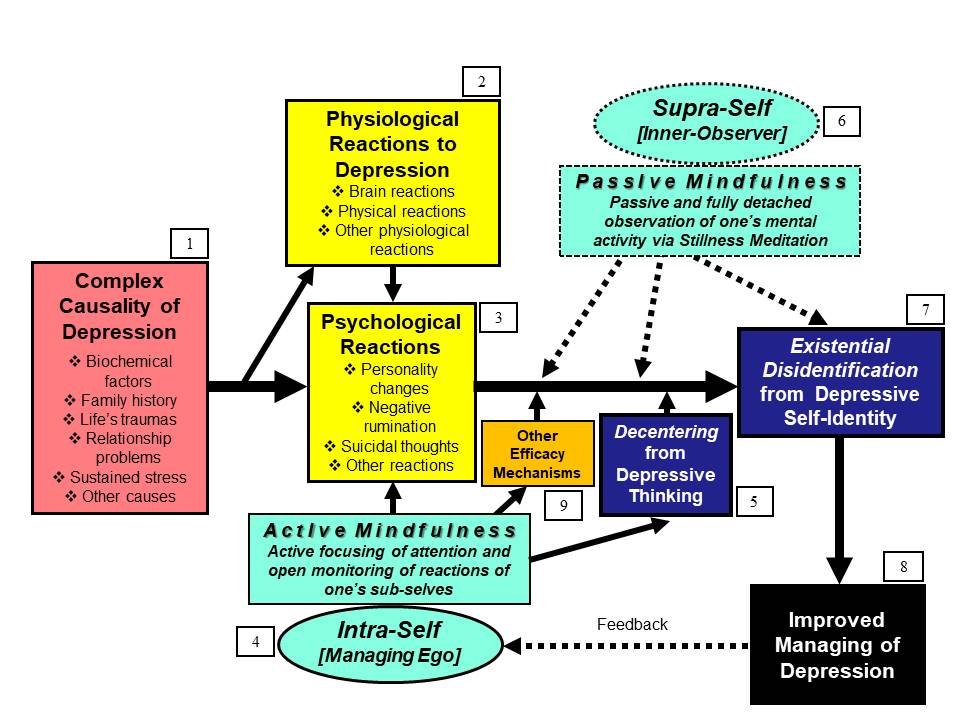
Figure 1 Binary model of the dynamics of mindfulness meditation in managing depression.
NB. The above binary model of active versus passive mindfulness is based on that advanced originally by Hede [80] to explain mindfulness in reducing executive stress. The central processes are posited to be the two modes of mindfulness, namely, active mindfulness and passive mindfulness (re-labelled from ‘meta-mindfulness’ and ‘supra-mindfulness’, respectively, which comprised Hede’s recent model [81] to explain how mindfulness can reduce the health effects of environmental noise on communities).
The following explanatory notes correspond with the numbered elements in the model above (see Figure 1):
[1] The causality of depression is known to comprise a complex of sources including various biochemical factors, sustained stress, as well as life factors including experiential traumas, relationship and family problems, as well as other causes [91] (see No.1 ‘Complex Causality of Depression’ in Figure 1).
[2] The first reactions that people experience in encountering depression are usually physiological. Of these, most people are likely to experience neuro-chemical reactions, physical fatigue, sleep disturbance, as well as a range of other physiological conditions. (see No.2 in Figure 1, ‘Physiological Reactions to Depression’).
[3] As well as physiological reactions, people suffering depression are prone to experience psychological reactions especially incessant negative thinking including possibly, suicidal thoughts. A useful summary provided by one source is as follows: “Most common symptoms of depression include sadness, dissatisfaction, spontaneous crying, irritability, withdrawal, increased tiredness, weight loss and lack of interest in sex” [92]. Note that psychological reactions may be subjectively experienced prior to or concurrent with physiological reactions but depression sufferers typically lack reflective awareness. (see No.3 ‘Psychological Reactions’ in Figure 1).
[4] The ‘intra-self’ operates within the mind and functions as one’s ‘managing ego’ (equivalent to the ‘aware ego’ [86]) which deals with manages the constant chatter of the ‘sub-selves’ (see No.4 in Figure 1, ‘Intra-Self’). The present model postulates that when an individual learns mindfulness, it is their ‘intra-self’ that acquires the capacity for ‘active-mindfulness’. This entails two mechanisms that assist with conditions such as depression, namely, focused attention and the active but non-judgmental monitoring of one’s own mental processes [78,89]. Thus, active mindfulness as a key function of one’s ‘intra-self’ is equivalent to the conceptualization of mindfulness which is dominant in the literature (see Section 4 above).
[5] As far as possible, the proposed binary model of mindfulness has been designed to incorporate elements previously validated in the literature. Thus, the mechanism with the greatest efficacy in relation to depression is here posited to be ‘decentering’ [90] (see No.5 in Figure 1, ‘Decentering from Depressive Thinking’). The process of ‘active mindfulness’ as proposed here, has been shown in many studies reviewed above to develop an individual’s capacity to detach from their own depressive thinking. The current model explains such thoughts as continuously fed to an individual in their ‘mindchatter’ by elements of their own mind, specifically, their sub-selves.
[6] The ‘supra-self’ is the ‘higher self’ of the human psyche (see No.6 in Figure 1, ‘Supra-Self: Inner Observer’). Whereas the ‘intra-self’ functions as one’s ‘managing ego’ which is actively involved in mental processes (as discussed in Point No.4 above), the ‘supra-self’ is an individual’s ‘inner observer’ whose function is completely passive and operates detached from mind (viz., in a state of ‘no mind’). This construct is comparable to Deikman’s notion of the ‘observing self’ [89].
[7] The primary mechanism whereby the ‘supra-self’ effects permanent change in an individual suffering from depression is via existential disidentification (see No.7 in Figure 1, ‘Existential Disidentification from Depressive Self-Identity’). This construct is called ‘existential disidentification’ because it relates to how one experiences one’s existence, to distinguish it from ‘cognitive disidentification’ which involves intellectual disengagement from one’s mental states.
[8] As depicted in the model (see No.8 in Figure 1, ‘Improved Managing of Depression’), it is hypothesized that by training themselves in both active and passive mindfulness, individuals can reduce the impact of depression in their lives. The use of the term ‘improved managing’ rather than ‘cure’ is intended to convey that major depression is likely to persist or recur in some form, but that the ongoing practice of mindfulness can prevent a serious relapse.
[9] The final element in the proposed binary model of mindfulness (see No.9 in Figure 1, ‘Other Efficacy Mechanisms’) is included because of the many efficacy mechanisms that have been identified in the literature (see Section 4 above). Also, future research is likely to further clarify precisely how mindfulness achieves its health benefits, both physiological and psychological.
6. Discussion
In evaluating the above model, it is essential to consider that that there is a long tradition in Psychology and Behavioral Medicine of ‘explaining’ a process by identifying its component constructs and also by showing how they interact (usually indicated by means of connecting lines in illustrative diagrams. This is exactly what the current proposed binary model does (see Figure 1 above). It is important to note that the proposed model is not attempting to explain all MBCT interventions but only the two-stage therapeutic intervention specified, namely, ‘decentering’ via active mindfulness by the ‘intra-self’ and ‘existential disidentification’ via passive mindfulness by the ‘supra-self’.
The binary model presented here is distinctive in that it posits a tripartite composition of the human psyche (viz., sub-selves, intra-self, supra-self) as well as two distinct mindfulness processes (active versus passive) by which these selves function in one’s everyday life. Like Freud’s famous tripartite model of personality (id, ego, superego) [85], the self components of the psyche as here proposed are definitely not ‘internal little men’ (from ‘homunculus’ in Latin) as the well-known philosophical theory argues [93]. Nor are they internal spirit beings but rather emergent functions whose existence can be inferred from their capacity to determine an individual’s recurrent behaviors rather like human functions such as intelligence, wisdom and selfishness. The proposed components of the psyche comprise firstly, the ‘sub-selves’ which are evidenced in every individuals’ constant ‘mindchatter’, plus secondly, the ‘intra-self’ or ‘managing ego’ which enables an individual to manage the complex activities of their mind especially the many voices of their sub-selves and also to interact with the outside world. The third and ultimate structural component of the psyche is posited to be the ‘supra-self’ which is every individual’s ‘higher self’ and which has the potential to function as their ‘inner observer’.
Whereas the ‘intra-self’ is postulated as an active entity, the ‘supra-self’ is a passive and largely overlooked component of one’s psyche. That is, it is only when an individual surrenders all control to the neutral observation by their supra-self (as during stillness meditation) that they can truly achieve a state of being ‘above mind’ in the sense of being fully detached from all mental activity. Importantly, the ‘supra-self’ either observes or it doesn’t. If it does observe, it takes no action for its function is purely neutral and passive. However, if the ‘supra-self’ doesn’t observe, it is completely non-functional and irrelevant to the individual’s life. In sharp contrast with homunculus theory, the current tripartite model of the human psyche does not entail endless levels of self ad infinitum. Rather, the proposed kinds of self (‘intra-self’ and ‘supra-self) are capable of engaging in two different modes of mindfulness, namely, active mindfulness in the case of the intra-self and passive mindfulness when it involves the supra-self. Note that the proposed distinction between two modes of mindfulness should improve our understanding of mindfulness in practice and may result in a more effective two-stage intervention for depression subject to empirical validation.
The main existing binary conceptualization of mindfulness in the literature seems to be that proposed 20 years ago by Martin who distinguished two forms of mindfulness based on their use of attention [94]. The first is an open form of mindfulness involving open attention while the second is a focused form of mindfulness involving focused attention. According to Martin: “The open form is like a space ship that can freely hover and examine a landscape. Once on the surface of a planet, focused-form attention is necessary to identify, spot, or follow a path to an alternate landscape.” [94]. Martin compares his binary conceptualization with various constructs proposed by others. For example, he draws an equivalence between his two attentional forms of mindfulness (open versus focused) and the Buddhist distinction between insight meditation (vipassanā) and concentration meditation (samadhi) [36,94]. Another example cited by Martin is Seeth’s distinction between two types of attention used by psychotherapists, namely, panoramic attention (open) versus narrow-focused attention (focused) [94,95]. Yet another binary classification is Deikman’s [89] notion of the ‘observing self’ which is posited to be capable of either a ‘receptive mode’ (= open) and an ‘object or action mode’ (= focused).
Let us adapt Martin’s spaceship analogy (see previous paragraph) in order to conduct a direct comparative analysis of his notion of binary attentional forms versus the present binary model of active versus passive mindfulness (see Figure 1). First, let’s summarize the two approaches starting with Martin’s distinction between two attentional forms of mindfulness (viz., open versus focused) which he provides without any information about the mental structures assumed to be involved [94]. By contrast, the present model distinguishes between active mindfulness (conducted by the ‘intra-self’ or ‘managing ego’ which operates totally in the mind) and passive mindfulness (which involves the presence of a completely passive ‘supra-self’ or ‘inner observer’ which operates ‘above’ and detached from the mindchatter of the mind). “As proposed here, the alternative to Martin’s spaceship hovers over the landscape within one’s mind actively searching for a landing site and scanning for any hostile mental activity especially the ‘mindchatter’ of the noisy locals (‘sub-selves’). Once the alternative spaceship has landed under the supervision of its pilot (‘managing ego’), it can close down all systems and allow its ‘neutral eye’ on its surveillance tower to observe all activity both inside and around the spaceship such that ‘stillness prevails’. Whenever an emergency arises, as happens often, the neutral ‘inner observer’ disengages and the pilot takes over full control initiating corrective mental activity as required.” (see Figure 1).
The first thing to notice from the allegorical spaceship comparison above is that the two attentional processes are opposites in the two models. Whereas Martin’s spaceship starts in open attention mode hovering above the landscape, the present model starts in active mindfulness mode searching for a landing site and scanning for local (mental) activity. Importantly, both models involve activity though Martin’s model clearly views ‘focused attention’ as involving more action than ‘open attention’ considering that he mentions ‘action’ several times in relation to focused attention (e.g., “A focused attentional form facilitates action…” [94]. The proposed binary mindfulness model, by contrast, posits a clear distinction between the mental activity of the intra-self (active mindfulness comprising both focused attention and open monitoring) as compared with the total passivity from the supra-self (passive mindfulness, that is, neutral observation without any form of mental activity).
As noted above, Martin cited a number of published conceptualizations equivalent to his notion of open versus focused attention. Interestingly, in the two decades since his article first appeared in 1997, there have been several other comparable models of mindfulness which distinguish focused attention versus open monitoring (see Section 4). All six of the conceptualizations of mindfulness reviewed here (viz., those proposed by: Martin [94], Speeth [95], Deikman [89], Bishop [69], Britton [78], and Lutz [79]), involve two active functions both of which are accommodated within the present construct of ‘active mindfulness’. Firstly, focused attention or its equivalent in the other models cited above, is clearly an active process requiring mental effort to sustain continuous focus and also to re-focus when the mind wanders [79,94]. According to Lutz et al., FA meditation (focused attention), “entails voluntary focusing of attention on a chosen object in a sustained fashion” [79]. These researchers posit that OM meditation (open monitoring), on the other hand, “involves nonreactively monitoring the content of experience from moment to moment, primarily as a means to recognize the nature of emotional and cognitive patterns” [79]. This view is shared by all the other models under consideration in this paper. Significantly, in the various models considered, open monitoring is viewed as less of an active process as compared with focused attention (see above), but is nevertheless an active process for as Lutz et al. point out regarding open monitoring, “there is also an increasing emphasis on cultivating (sic) a ‘reflexive’ awareness that grants one greater access to the rich features of each experience” [79]. It is argued here, that this contrasts with the current binary model which hypothesizes that passive mindfulness involves nothing but neutral inner stillness without any mental activity (see Figure 1).
As proposed in the current binary model, the two modes of mindfulness (active versus passive) are primarily linked to two efficacy mechanisms involving the ‘intra-self’ (managing ego) and the ‘supra-self’ (inner observer), namely, decentering and existential disidentification, respectively (see Figure 1). These are two of the many related constructs proposed in the literature which Bernstein et al. list alphabetically as follows: cognitive defusion (or deliteralization); cognitive distancing; decentering; detached mindfulness; meta-cognitive awareness; metacognitive mode; mindfulness; reperceiving; self-as-context; and self-distanced perspective [96,p.600]. While diverse in their detail, these metacognitive processes all relate to the very human capacity “to shift experiential perspective – from within one’s subjective experience onto that experience”, a capacity these researchers describe broadly as “decentering” [96]. Bernstein et al. also propose a model of decentering which comprises three constructs, namely, 1) meta-awareness, (awareness of subjective experience), 2) disidentification from internal experience (the experience of internal states as separate from one’s self), and 3) reduced reactivity to thought content (reduced effects of thought content on other mental processes) [96].
The second key mechanism endorsed in the present model is the efficacy process of existential disidentification. It is notable that most of the psychological literature on disidentification deals with self-identity in relation to social factors such as nationality, race, occupation, organization [e.g., 98]. Bernstein et al. define ‘disidentification’ as the capacity to experience one’s own internal activities and states as distinct from one’s own existential self. As they assert: “This experiential disidentification contrasts with the human tendency to identify with subjective experience and, therein, to experience internal states such as thoughts, emotions, and sensations as integral parts of the self.” [96]. As an example, if a depressed person experiences the thought ‘I’m worthless’ they may be tempted to interpret this as confirmation that they are indeed, a worthless being, and to further argue ‘because my infallible mind tells me so and, therefore, it must be true’). Similarly for all the thoughts listed in the published automatic thoughts questionnaire [97] which provides an authoritative measure of depressive thinking. Disidentification enables the person to realise as they happen that their automatic (negative) thoughts are simply events in their mind, indeed, that they are no different from the other ‘mindchatter’ that their ‘sub-selves’ voice continually. But so-called ‘automatic thoughts’ become problematic for the depressed person not so much when they are continuously repeated as intellectual assertions but more so when such thoughts become integrated into one’s self-identity. There are many techniques aimed at reducing the impact of negative thinking, for example, the long-established method of cognitive defusion adopted by Acceptance and Commitment Therapy (ACT) entails the rapid repetition of a single word [99]. Thus, a depressed person might identify the negative thought they find most disturbing as being ‘I’m always sad’ and from this they might derive the word ‘sad’ for repetition. By repeating this word its semantic meaning eventually becomes less dominant or ‘defused’ and their attachment to the literal meaning of their unwanted thought becomes less believable and, hence, more manageable [99].
From the previous discussion, there appear to be two relevant types of disidentification which are here labelled cognitive versus existential. The first, as addressed in the model advanced by Bernstein and associates [96], is the capacity to process one’s mental experiences as they occur such that they are interpreted as events and states that are happening in one’s mind rather than as occurrences that directly reflect one’s existential self. In the present binary model, cognitive disidentification is a mental skill that can be acquired, albeit with much training and effort, by using the resources of the ‘managing ego’ (intra-self). For a depressed individual, it is primarily the ‘sub-selves’ (especially ‘The Miserable’ and ‘The Critic’ or similar – see Section 5), who collude not only in repeating negative slogans (such as those from the official list of automatic thoughts [97]), but who are well-practiced at engaging the ‘intra-self’ in debate about how the person’s thoughts are evidence of their depressed existence. Of course, it is a great cognitive skill to be able to process one’s negative or unpleasant mental events in the present moment without their affecting one’s self-identity and sense of being.
The second type of disidentification (viz., existential) is much more difficult to manage in practice because it requires the depressive individual to acquire a profound existential insight (specifically, a fundamental shift in one’s deep conviction about who one really is). As we have seen, cognitive disidentification enables a person with depression, to learn various cognitive skills (decentering, defusion etc.) which empower them to experience their mental states without affecting their sense of existence [100,101]. While existential disidentification, on the other hand, is difficult to achieve in practice, but the underlying logic is straightforward, namely: ‘I observe my mind; therefore, I cannot be my mind’. As one practices stillness meditation, their supra-self (‘inner observer’) engages in passive mindfulness such that they eventually experience their mind as being distinct from their existence. No amount of mental effort, intellectual repetition or cognitive assertion can produce a shift in one’s sense of core identity. For a person who has lived many years struggling with their self-identity as a depressive person, the best they can hope for is metacognitive awareness involving active mindfulness. As Teasdale and colleagues proposed some 15 years ago, “Metacognitive awareness is a cognitive set in which negative thoughts/feelings are experienced as mental events, rather than as the self” [102]. But even if new mental events are not experienced as the self because of active mindfulness, the depressive person’s self-identity is already locked in and cannot be changed except via an existential shift (specifically, via existential disidentification).
However, because the supra-self is totally confined to passive observation during stillness meditation, it is not able to actively intervene in the process of existential disidentification. It’s rather like a child attempting to catch a soap bubble – the very attempt simply bursts the bubble. In practice, the main aim of disidentification in the treatment of depression is to change both one’s way of dealing with negative thoughts (cognitive) as well as shifting one’s self-identity from that of a depressive to that of a being who exists beyond one’s mind) (existential) (i.e., one’s ‘inner observer’ – see Figure 1). With another nod to Descartes, any person may reason: ‘I think; therefore, I must have a mind.’ This assertion makes a simple logical point, namely, that if I think, I must have a mind which does the thinking. However, the person can take the next logical step of realising another assertion that: ‘Because I can observe my mind operating separately, therefore, I am not my mind’. This second assertion, on the other hand, is not logically derived from the first assertion but is rather a distinct insight gained from reflecting on one’s own mental experience, that is, an ‘aha’ moment about one’s true existence as separate from one’s ‘mindchattery’ mind.
The final issue to consider is how the present binary model of mindfulness stands up to empirical investigation. Such a study could be designed by randomly assigning approximately 120 depression sufferers to one of three test conditions based on the 8-week MBCT course [60,103], namely, a) standard MBCT course (as an active control); b) MBCT course with special emphasis on active mindfulness and defusion; c) MBCT course with special emphasis on passive mindfulness and existential disidentification; d) MBCT course with special emphasis on both defusion and existential disintegration (see Figure 1). The outcome measures could include the following: 1) pre and post scores on the Beck Depression Inventory [63]; 2) relapse and recurrence rates of depression across the test conditions after 6 and 12 months [63]; 3) other measures based on specific literature review. Comparisons among the four test groups would indicate the specific efficacy of the mindfulness mechanisms.
7. Conclusions
In order to introduce a new conceptual model comprising two modes of mindfulness (active versus passive) within a new tripartite framework of the psyche-as-selves, the current review aimed to assess mindfulness from the historical, empirical and theoretical viewpoints. It has been shown that there exists evidence across many studies and empirical meta-analyses for the efficacy of mindfulness in treating a range of physiological and psychological conditions, particularly depression. Further, although there are a rich variety of conceptual models describing the mindfulness efficacy mechanisms involved, there is no consensus yet in the literature. However, this paper has acknowledged that there is a strong body of opinion which questions the overall validity of the mindfulness approach to therapeutic intervention and points to the need for more rigorous methodology in future [82,84].
Nevertheless, it has been shown here that a number of themes are emerging regarding, for example, types of meditation (focused attention versus open monitoring) and types of awareness (meta-cognitive awareness and cognitive disidentification). This paper has presented a tripartite model of the human psyche comprising: 1) the sub-selves which are responsible for the constant ‘mindchatter’ that clutter one’s mind, 2) the ‘intra-self’ (one’s managing ego) which engages in active mindfulness works to manage the ongoing chaos of one’s mind on a daily basis, and 3) the ‘supra-self’ (one’s inner observer) which engages in passive mindfulness to neutrally monitor all of one’s mental activity without offering any judgment or control. The present binary model posits that both active mindfulness and passive mindfulness need to be accessed in order to gain the maximum benefit in managing depression. The various cognitive techniques which are becoming accepted in psychological practice [103], are accessible to the intra-self (managing ego) via active mindfulness (see Figure 1). But potentially the most effective efficacy mechanism in the case of depression is existential disidentification which helps a depression sufferer to re-define their sense of self-identity so that they can avoid interpreting everything in their lives as confirming their depressive existence. This is the key hypothesis that needs to be tested in future research on the proposed binary model of mindfulness by comparing the outcomes for depression sufferers randomly assigned to different conditions of 8-week MBCT training.
Acknowledgments
The University of the Sunshine Coast (Australia) supported this research by providing full access to their library and database resources.
Author Contributions
The author is solely responsible for the writing, revising and approving of this manuscript for publication.
Competing Interests
The author has declared that no competing interests exist in this work.
References
- Pollitt J. Suggestions for a physiological classification of depression. Br J Psychiatry. 1965; 111: 489-495. [CrossRef]
- World Health Organization. Factsheets – Depression. 2018, 29 April; Available from: http://www.who.int/mediacentre/factsheets/fs369/en/.
- American Psychiatric Association. What is depression? 2018, 11 June; Available from: https://www.psychiatry.org/patients-families/depression/what-is-depression.
- Wood J. Antidepressant use up 400 percent in US. PsychCentral. 2011, 30 October; Available from: https://psychcentral.com/news/2011/10/25/antidepressant-use-up-400-percent-in-us/30677.html.
- Kuyken W, Hayes R, Barrett B, Byng R, Dalgleish T, Kessler D, et al. Effectiveness and cost-effectiveness of mindfulness-based cognitive therapy compared with maintenance antidepressant treatment in the prevention of depressive relapse or recurrent (PREVENT): a randomised controlled trial. Lancet. 2015; 386: 63-73. [CrossRef]
- Reimann D, Hertenstein E, Schramm E. Mindfulness-based cognitive therapy for depression. Lancet. 2016; 387: 1054. [CrossRef]
- Kabat-Zinn J. Some reflections on the origins of MBSR, skillful means, and the trouble with maps. Contemp Buddhism. 2011; 12: 281-306. [CrossRef]
- Kabat-Zinn J. Wherever you go, there you are: Mindfulness meditation in everyday life, New York NY: Hyperion, 1994.
- Kabat-Zinn J. Full catastrophe living: Using the wisdom of your body and mind to face stress, pain and illness. New York NY: Bantam Dell; 1990.
- Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J Psychosom Res. 2004; 57: 35-43. [CrossRef]
- Mackenzie MB, Kocovski NL. Mindfulness-based cognitive therapy for depression: trends and developments. Psychol Res Behav Manag. 2016; 9: 125-132.
- Mason O, Hargreaves I. A qualitative study of mindfulness-based cognitive therapy for depression. Br J Med Psychol. 2001; 74: 197-212. [CrossRef]
- Blanck P, Perleth S, Heidenreich T, Kroger P, Ditzen B, Bents H, et al. Effects of mindfulness exercises as stand-alone intervention on symptoms of anxiety and depression: Systematic review and meta-analysis. Behav Res Ther. 2018; 102: 25-35. [CrossRef]
- Lo HH, Ng SM, Chan CL, Lam KF, Lau BH. The Chinese medicine construct ‘stagnation’ in mind-body connection mediates the effects of mindfulness training on depression and anxiety. Complement Ther Med. 2013; 1: 348-57. [CrossRef]
- Lahera G, Bayon C, Fe Bravo-Ortiz M, Rodriguez-Vega B, Barbeito S, Saenz M, et al. Mindfulness-based cognitive therapy versus psychoeducational intervention in bipolar outpatients with sub-threshold depressive symptoms: a randomized controlled trial. BMC Psychiatry. 2014; 14: 215-22. [CrossRef]
- Ives-Deliperi VI, Howells F, Stein DJ, Mientjes EM, Horn M. The effects of mindfulness-based cognitive therapy in patients with bipolar disorder: A controlled functional MRI investigation. J Affect Disord. 2013; 150: 1152-1157. [CrossRef]
- Kabat-Zinn J. An outpatient program in behavioural medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen Hosp Psychiat. 1982; 4: 33-47. [CrossRef]
- Hilton, L, Hempel S, Ewing B, Apaydin E, Xenakis L, Newberry S, et al. Mindfulness meditation for chronic pain: Systematic review and meta-analysis. Ann Behav Med. 2017, 51: 199-213. [CrossRef]
- Fitzpatrick L, Simpson J, Smith A. A qualitative analysis of mindfulness-based cognitive therapy (MBCT) in Parkinson’s disease. Psychol Psychother. 2010; 83: 179-192. [CrossRef]
- Advocat J, Russell G, Enticott J, Hassad C, Hester J, Vandenberg B. The effects of a mindfulness-based lifestyle programme for adults with Parkinson’s disease: protocol for a mixed methods, randomised two-group control study. BMJ Open. 2013; 3: 1-8. [CrossRef]
- Chan J, Clarke AC, Royan L, Stott J, Spector A. A mindfulness program manual for people with dementia. Beh Modif. 2017; 41: 764-787. [CrossRef]
- Tang V, Wai SP, Kwan P. Mindfulness-based therapy for drug-resistant epilepsy: An assessor-blinded randomized trial. Neurology. 2015; 85: 1100-1107. [CrossRef]
- Simpson R, Booth J, Lawrence M, Byrne S, Mair F, Mercer S. Mindfulness based interventions in multiple sclerosis – a systematic review. BMC Neurol. 2014; 14: 15-23. [CrossRef]
- Tavee J, Stone L. Healing the mind: Meditation and multiple sclerosis. Neurology. 2010; 75: 1130-1131. [CrossRef]
- Eifring H. Meditation in Judaism, Christianity and Islam: Cultural histories. London: Bloomsbury; 2015.
- Eifring H. Hindu, Buddhist and Daoist Meditation: Cultural Histories. New York NY: Hermes Academic; 2014.
- Eifring H. Characteristics of East Asian meditation. Acta Orientalia. 2010; 71: 125-157.
- Gunaratana BH. Mindfulness in plain English. Somerville MA: Wisdom Publications; 2002.
- Nhat Hanh T. The Miracle of mindfulness: An introduction to the practice of meditation. Boston MA: Beacon Press; 1975.
- Chumley N. Mysteries of the Jesus prayer: Experiencing the presence of god and a pilgrimage to the heart of an ancient spirituality. San Francisco CA: HarperOne; 2011.
- Chan R. Mantra meditation as a bedside spiritual intervention. Medsurg Nurs. 2014; 23: 84-88.
- Encyclopedia Britannica. Schism of 1054. 2018, 30 April; Available from: https://www.britannica.com/event/Schism-of-1054.
- Anonymous. The way of a pilgrim: And the pilgrim continues his way, 2nd ed. Pasadena CA: Hope Publishing House; 1989.
- Mathewes-Green F. The Jesus prayer: The ancient desert prayer that tunes the heart to god. Orleans MA: Paraclete Press; 2009.
- Main J. Word into silence: A manual for Christian meditation. Norwich England: Canterbury Press; 2006.
- Gethin, R. On some definitions of mindfulness. Contemp Buddhism. 2011; 12: 263-279. [CrossRef]
- Shonin E, Van Gordon W, Singh NN, eds. Buddhist foundations of mindfulness. Cham, Switzerland: Springer International Publishing; 2015. [CrossRef]
- Kuan TF. Mindfulness in early Buddhism: New approaches through psychology and textual analysis of Pali, Chinese and Sanskrit sources. London: Routledge; 2008.
- Thera S. The way of mindfulness: The Satipatthana Sutta and its commentary. Kandy, Sri Lanka: Buddhist Publication Society; 1967, 1949, 1941.
- Nanamoli B. Mindfulness of breathing (Anapanasati). Kandy, Sri Lanka: Buddhist Publication Society; 1952.
- Bullen L. Buddhism: A method of mind training. Bodhi Leaves No: 42. Kandy, Sri Lanka: Buddhist Publication Society; 1965.
- Thurman RAF. Meditation and education: India, Tibet and modern America. Teachers College Record. 2006; 108: 1765-1774. [CrossRef]
- Heffernan, V. The muddled meaning of ‘mindfulness’. The New York Times Magazine. First Words. 2015, 14 April.
- Bodhi, B. What does mindfulness really mean? A canonical perspective. Contemp Buddhism. 2011; 12: 19-39. [CrossRef]
- Segal ZV, Williams JM, Teasdale JD. Mindfulness-Based Cognitive Therapy for depression: A new approach to preventing relapse. New York, NY: Guilford Press; 2002.
- Teasdale JD, Segal ZV, Williams MG, Ridgeway VA, Soulsby JM, Lau, MA. Prevention of relapse/recurrence in major depression by Mindfulness-Based Cognitive Therapy. J Consult Clin Psychol. 2000; 68: 615-623. [CrossRef]
- Mindfulness-Based Stress Reduction – MBSR. Centre for Mindfulness, University of Massachusetts Medical School. May 2018; Available from: https://www.umassmed.edu/cfm/mindfulness-based-programs/mbsr-cou rses/mbsr/.
- Harris R. Medical practitioner, psychotherapist, life coach. August 2018, Available from: https://www.actmindfully.com.au/about-russ/.
- McCabe JA, Freidman-Wheeler DG. Mindfulness and meditation in Psychology courses. Society for the Teaching of Psychology: Division 2 of the American Psychological Association. Dec 2017; Available from: https://teachpsych.org/E-xcellence-in-Teaching-Blog/5611996.
- Harris R. Mindfulness without meditation. Healthc Counsel Psychoth J. 2009; Oct: 21-24.
- AMRA. Mindfulness journal publications by year, 1980-2017. American Mindfulness Research Association. March 2018; Available from: https://goamra.org/resources/.
- Fisher D. Mindfulness and the cessation of suffering: An exclusive new interview with mindfulness pioneer Jon Kabat-Zinn. October 2010; Available from: https://www.lionsroar.com/mindfulness-and-the-cessation-of-suffering-an-exclusive-new-interview-with-mindfulness-pioneer-jon-kabat-zinn/.ool.
- Kabat-Zinn J, Lipworth L, Burney R. The clinical use of mindfulness meditation for the self-regulation of chronic pain. J Behav Med. 1985; 8: 163-190. [CrossRef]
- Gotink RA, Meijboom R, Verwooij, MW, Smits M, Myriam Hunink. 8-week mindfulness-based stress reduction induces brain changes similar to traditional long-term meditation practice – A systematic review. Brain Cogn. 2016; 108: 32-41. [CrossRef]
- Kabat-Zinn J. Full Catastrophe Living Summary. 2018 June; Available from: https://www.getnugget.co/full-catastrophe-living-summary/.
- Chiesa A, Serretti A. Mindfulness-based stress reduction for stress management in healthy people: A review and meta-analysis. J Altern Complement Med. 2009; 15: 593-600. [CrossRef]
- Khoury B, Sharma M, Rush S, Fournier C. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J Psychosom Res. 2015; 78: 519-528. [CrossRef]
- Gotink RA, Chu P, Busschbach JJV, Benson H, Fricchione L, Hunink MGM. Standardised mindfulness-based interventions in healthcare: An overview of systematic reviews and meta-analyses of RCTs. PLoS One. 2015; 10: 1-17. [CrossRef]
- Butler AC, Chapman JE, Forman EM, Beck AT. The empirical status of cognitive-behavioral therapy: A review of meta-analyses. Clin Psychol Rev. 2006; 26: 17-31. [CrossRef]
- A mindful way through depression – MBCT. Centre for Mindfulness, University of Massachusetts Medical School. June 2018; Available from: https://www.umassmed.edu/cfm/mindfulness-based-programs/mbct-courses/mbct/.
- Dobson KS, Duzois DJA. Historical and philosophical bases of the cognitive-behavioral therapies. In: Dobson KS ed. Handbook of Behavioral Therapies. 3rd ed. New York, NY: Guilford Press; 2009. 3-38.
- Reynolds WM, Coats KI. A comparison of cognitive-behavioral therapy and relaxation training for the treatment of depression in adolescents. J Consult Clin Psychol. 1986; 54: 653-660. [CrossRef]
- Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin Psychol Rev. 1988; 8: 77-100. [CrossRef]
- Chiesa A, Serretti A. Mindfulness-based cognitive therapy for psychiatric disorders: A systematic review and meta-analysis. Psychiat Res. 2011; 187: 441-453. [CrossRef]
- Clarke K, Mayo-Wilson E, Kenny J, Pilling S. Can non-pharmacological interventions prevent relapse in adults who have recovered from depression? A systematic review and meta-analysis of randomised controlled trials. Clin Psychol Rev. 2015; 39: 58-70. [CrossRef]
- Kuyken W, Warren FC, Taylor RS, Whaley B, Crane C, Bondolfi G, et al. Efficacy of mindfulness-based cognitive therapy in prevention of depressive relapse: An individual patient data meta-analysis from randomized trials. JAMA Psychiatry. 2016; 73: 565-574. [CrossRef]
- Oxford Mindfulness Centre. MBCT for recurrent depression: What do we know? What does it mean? Where to next? October 2016; Available from: http://oxfordmindfulness.org/news/mbct-recurrent-depression-know-mean-next/.
- Baer RA. Mindfulness training as a clinical intervention: A conceptual and empirical review. Clin Psychol-Sci Pr. 2003; 10: 125-143. [CrossRef]
- Bishop SR, Lau M, Shapiro S, Carlson L, Anderson ND, Carmody J, et al. Mindfulness: A proposed operational definition. Clin Psychol-Sci Pr. 2004; 11: 230-241. [CrossRef]
- Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. 2006; 13: 27-45. [CrossRef]
- Teper R, Segal ZV, Inzlicht M. Inside the mindful mind: How mindfulness enhances emotion regulation through improvements in executive control. Curr Dir Psychol Sci. 2013; 20: 1-6. [CrossRef]
- Brown KW, Ryan RM, Creswell JD. Mindfulness: Theoretical foundations and evidence for its salutary effects. Psychol Inq. 2007; 18: 211-237. [CrossRef]
- Gu J, Strauss C, Bond R, Cavanagh K. How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of meditation studies. Clin Psychol Rev. 2015; 37: 1-12. [CrossRef]
- Garland EL, Gaylord S, Park J. The role of mindfulness in positive reappraisal. Explore (NY). 2009; 5: 37-44. [CrossRef]
- Van der Velden AM, Kurken W, Wattar U, Crane C, Pallesen KJ, Dahlgaard J, et al. A systematic review of mechanisms of change in mindfulness-based cognitive therapy in the treatment of recurrent major depressive disorder. Clin Psychol Rev. 2015; 37: 26-39. [CrossRef]
- Lindsay EK, Creswell JD. Mechanisms of mindfulness training: Monitor and acceptance theory (MAT). Clin Psychol Rev. 2017; 51: 48-59. [CrossRef]
- Alsubaie M, Abbott R, Dunn B, Dickens C, Kell TF, Henley W, et al. Mechanisms of action in mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR) in people with physical and/or psychological conditions: A systematic review. Clin Psychol Rev. 2017; 55: 74-91. [CrossRef]
- Britton WB, Davis JH, Loucks EB, Peterson B, Cullen BH, Reuter L, et al. Dismantling Mindfulness-Based Cognitive Therapy: Creation and validation of 8-week focused attention and open monitoring interventions within a 3-armed randomized controlled trial. Behav Res Ther. 2018; 101: 92-107. [CrossRef]
- Lutz A, Slagter HA, Dunne JD, Davidson RJ. Attention regulation and monitoring in meditation. Trends in Cognitive Sciences. 2008; 12: 163-169. [CrossRef]
- Hede AJ. The dynamics of mindfulness in managing emotions and stress. J Manag Devel. 2010; 22: 25-39. [CrossRef]
- Hede AJ. Using mindfulness to reduce the health effects of community reaction to aircraft noise. Noise Health. 2017; 19: 165-173 [CrossRef]
- Van Dam NT, van Vugt MK, Vago DR, Schmalzl L, Saron CD, Olendzi A, et al. Mind the hype: A critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspect Psychol Sci. 2018; 13: 36-61. [CrossRef]
- Davidson RJ, Dahl CJ. Outstanding challenges in scientific research on mindfulness and meditation. Perspect Psychol Sci. 2018; 13: 62-65. [CrossRef]
- Van Dam NT, van Vugt MK, Vago DR, Schmalzl L, Saron CD, Olendzi A, et al. Reiterated concerns and further challenges for mindfulness and meditation research: A reply to Davidson and Dahl. Perspect Psychol Sci. 2018; 13: 66-69. [CrossRef]
- Cherry, K. The structural model of personality. 2017 Aug; Available from: https://www.verywellmind.com/the-id-ego-and-superego-2795951.
- Stone H, Stone S. Embracing our selves: The voice dialogue manual. Novato CA: New World Library; 1989.
- Dyak M. The voice dialogue facilitator’s handbook. Seattle WA: L.I.F.E. Energy Press; 1999.
- Tolle E. The power of now. Sydney: Hodder; 1999.
- Deikman, AJ. The observing self. Boston MA: Beacon Press; 1982.
- Aronson J, Blanton H, Cooper J. From dissonance to disidentification: Selectivity in the self-affirmation process. J Pers Soc Psychol. 1995; 68: 986-996. [CrossRef]
- Kanter JW, Busch AM, Weeks CE, Landes SJ. The nature of clinical depression: Symptoms, syndromes, and behavior analysis. Behav Anal. 2008; 31: 1-21. [CrossRef]
- Barakoti B, Jaiswal M, Adhikari B, Shyangwa PM. Depression in medical students. Kathmandu Univ Med J. 2012; 1: 45-46. [CrossRef]
- Lörincz A. Hebbian constraint on the resolution of the Homunculus Fallacy leads to a network that searches for hidden cause-effect relationships. Second conference on artificial general intelligence. Arlington VA: AGI-09; 2009, March. [CrossRef]
- Martin JR. Mindfulness: A proposed common factor. J Psychother Integr. 1997; 7: 291-312. [CrossRef]
- Speeth KR. On psychotherapeutic attention. J Transpers Psychol. 1982; 14: 141-160.
- Bernstein A, Hadash Y, Lichtash Y, Tanay G, Shepherd K, Fresco DM. Decentering and related constructs: A critical review and metacognitive processes model. Perspect Psychol Sci. 2015; 10: 599-617. [CrossRef]
- Hollon SD, Kendall PC. Cognitive self-statements in depression: Development of an automatic thoughts questionnaire. Cogn Ther Res. 1980; 4: 383–395. [CrossRef]
- Jasinskaja-Lahti I, Liebkind K, Solheim E. To identify or not to identify? National disidentification as an alternative reaction to perceived ethnic discrimination. Appl Psychol. 2009; 58: 105-128. [CrossRef]
- Matsuda A, Hayes SC, Sackett CF, Twohig MP. Cognitive defusion and self-relevant negative thoughts: examining the impact of a ninety year old technique. Behav Res Ther. 2004; 42: 477-485. [CrossRef]
- Larsson A, Hooper N, Osborne LA, Bennett P, McHugh L. Using brief cognitive restructuring and cognitive defusion techniques to cope with negative thoughts. Behav Modif. 2015; 40: 452-482. [CrossRef]
- Naragon-Gainey K, DeMarree KG. Structure and validity of measures of decentering and defusion. Psychol Assess. 2017; 29: 935-954. [CrossRef]
- Teasdale JD, Moore RG, Hayhurst H, Pope M, Williams S, Segal ZV. Metacognitive awareness and prevention of relapse in depression: Empirical evidence. J Consult Clin Psychol. 2002; 70: 275-287. [CrossRef]
- Teasdale J, Williams M, Segal Z. The mindful way workbook: An 8-week program to free yourself from depression and emotional distress. New York NY: The Guilford Press; 2014.
