

Perspectives on the Neurobiology of Antipsychotic Drugs in Psychiatric Disorders
Jenny Berrío 1 ![]() , Weiwen Wang 2
, Weiwen Wang 2![]() , Bart A. Ellenbroek 3,*
, Bart A. Ellenbroek 3,*![]()
- PPG-Ciências da reabilitação, Universidade Federal de Ciências da Saúde de Porto Alegre, Rua Sarmento Leite, 245, Porto Alegre, Brazil
- CAS Key Laboratory of Mental Health, Institute of Psychology, Beijing 100101, China
- School of Psychology, Victoria University of Wellington, Kelburn, Wellington 6012, New Zealand
* Correspondence: Bart A. Ellenbroek ![]() .
.
Received: January 18, 2017 | Accepted: February 27, 2017 | Published: March 15, 2017
OBM Neurobiology 2017, Volume 1, Issue 1, doi:10.21926/obm.neurobiol.1701001
Academic Editor: Hermes H. Yeh
Recommended citation: Berrío J, Wang W, Ellenbroek BA. Perspectives on the Neurobiology of Antipsychotic Drugs in Psychiatric Disorders. OBM Neurobiology 2017; 1(1): 001; doi:10.21926/obm.neurobiol.1701001.
© 2017 by the authors. This is an open access article distributed under the conditions of the Creative Commons by Attribution License, which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is correctly cited.
Abstract
Antipsychotics have been a pillar in the treatment of schizophrenia since their introduction more than 60 years ago. Their variety in structures and receptor binding properties confers on them a complex clinical profile of effectiveness and risk of adverse side-effects. Although antipsychotics are best known for their therapeutic effects in schizophrenia, these are limited to the positive symptoms, with much less influence on negative symptoms or cognitive deficits. Moreover, although the newer (so-called second-generation) antipsychotics were thought to have superior clinical profiles, this opinion has been undermined by most recent large-scale studies and meta-analyses. In fact, the beneficial effects of all antipsychotic drugs in the treatment of schizophrenia are remarkably similar, with the possible exception of clozapine. However, some evidence suggests differences in the side-effect profiles between the first- and second-generation drugs. Moreover, several of the second-generation antipsychotics are now also approved for several other conditions, such as bipolar disorder and autism spectrum disorders. In this review, we discuss the clinical usefulness of antipsychotics, their possible mode of action and describe the limitations of their use.
Keywords
Dopamine; Schizophrenia; Bipolar Disorder; treatment-resistant depression; Autism spectrum disorder; off-label use
Introduction
In the 1950s the biological approach to studying brain disorders was booming, with numerous breakthroughs in psychopharmacology, including the development of the first antidepressants (iproniazid and imipramine), the first anxiolytic (chlordiazepoxide) and the first antipsychotic (chlorpromazine). The introduction of chlorpromazine, which substantially improved the clinical course of schizophrenia rather than serving purely as a sedative, or even a “chemical” constraint, was seen as a major advance and led to the Lasker prize being awarded to Pierre Deniker in 1957 [1].
Chlorpromazine was the pioneer psychopharmacological drug of its kind. It was introduced as part of an anesthetic “cocktail” by the French anesthesiologist Henri Laborit, who quickly noted that it led to a state of “disinterestedness” in external events [2,3]. These effects attracted the attention of the French psychiatrists Jean Delay and Pierre Deniker, who began to administer chlorpromazine to their patients exhibiting altered states of excitation [4]. Intriguingly, the behavioral disturbances and psychotic symptoms of these patients lessened following the treatment without a concomitant sedative state or alteration in intellectual faculties. In fact, the psychiatrists noted a remarkable calming effect and excellent tolerability. These observations were replicated by other contemporary psychiatrists and soon it became clear that chlorpromazine was much more than a sedative and was capable of selectively reducing the psychotic symptoms in schizophrenic patients [5].
The subsequent and rapid spread of the use of chlorpromazine around the world led to the development of similar compounds, and at the same time, the recognition of undesired Parkinson-like motor symptoms and akathisia (extrapyramidal symptoms, EPS) among treated patients [6,7]. The notion that the therapeutic effects were a milder form of the neurological side-effects (“neuroleptic threshold”) emerged and was widely accepted for many years [8]. It was not until the therapeutic properties were shown to occur quite independently of the tendency to produce side-effects that this idea was abandoned. Among the new drugs introduced, clozapine represented an important example of this concept by standing out as a uniquely efficacious treatment for schizophrenia that was virtually devoid of any EPS. Because of this virtual lack of EPS, clozapine was termed an “atypical antipsychotic” as opposed to the “typical” or “classical” antipsychotics. Although this terminology is still in use today, we prefer first- and second-generation antipsychotics, since the evidence of a qualitative difference between these two classes of drugs is far from convincing (see below).
A crucial period in the history of antipsychotic drugs (as they were now generally referred to) was the voluntary withdrawal of clozapine after several deaths in Finland due to agranulocytosis [9]. This was followed by its re-introduction after the publication of a landmark report confirming its superiority over chlorpromazine [10]. During the intervening period, virtually no new antipsychotics were introduced. However, since the re-introduction of clozapine, numerous new drugs have successfully reached the market, further strengthening the distinction between first- and second-generation antipsychotics [11].
As a result, a large number of antipsychotic drugs are now used worldwide. Moreover, clinical studies have provided convincing evidence that certain antipsychotics are also beneficial for other mental disorders, including major depressive disorder, bipolar disorder, and autism spectrum disorders. Here, we review the clinical use of antipsychotic drugs in psychiatry and discuss the possible underlying biological mechanisms of action.
Antipsychotic Drugs
Before discussing the clinical and preclinical effects of antipsychotics, it is important to present a brief discussion of the diversity in their chemical structures and how this impacts on their basic pharmacological properties.
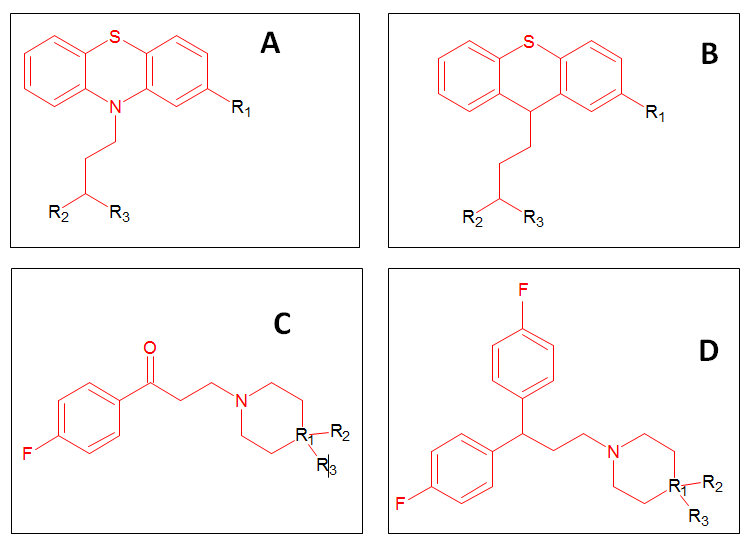
Figure 1 The chemical structures of the main classes of first-generation antipsychotics (FGAs) (A: the phenothiazines; B: the thioxanthenes; C: the butyrophenones; D: the diphenylbutylamines).
The first-generation antipsychotics (FGAs) are a large family of drugs with high lipophilicity, protein binding ability and large distribution volumes. Several have a long half-life but may undergo extensive first-pass metabolism by the liver, which makes their oral bioavailability highly variable and, in turn, leads to difficulties in establishing the correct dose for each patient. Most FGAs belong to four main chemical classes (see Figure 1): phenothiazines (including chlorpromazine, fluphenazine, thioridazine and perphenazine); thioxanthenes (including thiothixene, chlorprothixene, zuclopenthixol and flupenthixol), butyrophenones (including haloperidol, trifluperidol and spiroperidol), and diphenylbutylamines (including pimozide, fluspirilene and penfluridol).
In contrast, the second-generation antipsychotics (SGAs) (see Figure 2) show more diversity and do not form easily defined chemical classes. Nonetheless there are structural similarities, especially between clozapine and olanzapine (and to a lesser degree asenapine and quetiapine). A special case is the benzamides group (Figure 2H), which encompasses not only FGAs (such as sulpiride) and SGAs (such as amisulpride), but also drugs used for other indications (such as the anti-emetic drug, metoclopramide, and the anti-dyskinetic drug, tiapride).
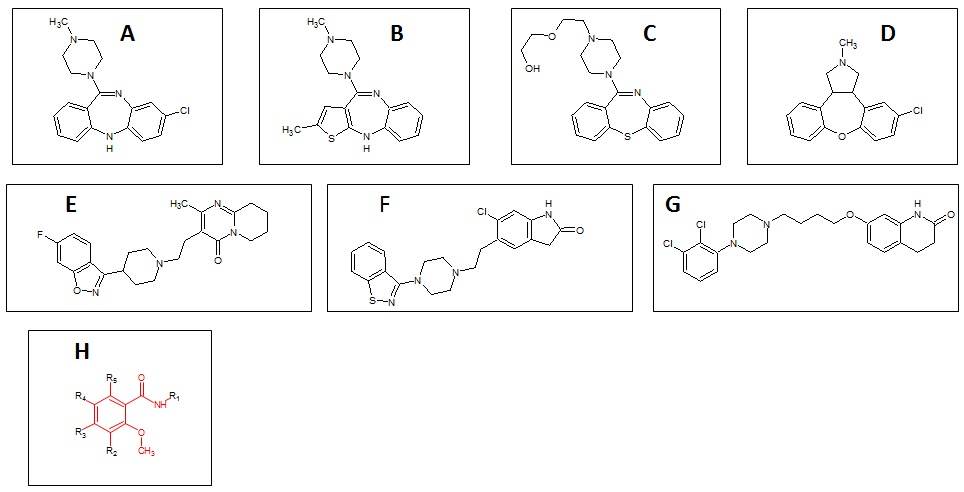
Figure 2 The chemical structure of the most important second-generation antipsychotics (SGAs) (A: clozapine; B: olanzapine; C: quetiapine; D: asenapine, E: risperidone; F: ziprasidone; G: aripiprazole. H: The chemical structure of the benzamides).
With such a multitude of antipsychotics from different chemical classes, it is not surprising that antipsychotics are known to influence many neurotransmitter systems. Indeed, with the exception of the benzamides, which show relatively high selectivity for the dopamine D2 receptor family, most antipsychotics have affinity for multiple receptors. Thus, the vast majority of antipsychotics block the dopamine D2, D3, and D4 receptors and the adrenergic α1, serotonergic 5-HT2A and 5-HT2C receptors. In addition, several antipsychotics potently block the dopamine D1, histamine H1 and serotonergic 5-HT7 receptors, while a few (most notably asenapine, chlorpromazine, clozapine and olanzapine) also block muscarinic acetylcholinergic receptors [11]. The relevance of these receptors to the therapeutic effects of these drugs and their side-effects is still not entirely clear, but will be discussed in more detail later in this review. However, we will first describe the therapeutic potential of antipsychotics for treating psychiatric disorders.
The Clinical Use of Antipsychotic Drugs
Schizophrenia
Schizophrenia is a severe psychiatric disorder characterized by the presence of three different classes of symptoms: positive (including hallucinations and delusions), negative (including anhedonia and social withdrawal) and cognitive symptoms (including deficits in attention, working memory and executive functioning). Like many other psychiatric disorders, its age of onset is shortly after puberty, typically 18–25 in men and 20–30 in women [12]. Although the etiology and pathology are still largely unknown, antipsychotic drugs have proved to be highly effective in the treatment of schizophrenia since their introduction in the 1950s and remain the drugs of choice for this disorder.
As a result of over 60 years of clinical experience with antipsychotic treatment, a tremendous amount of data has been accumulated on the therapeutic efficacy of these drugs in schizophrenia. In most recent studies, symptomatology is measured using the PANSS (Positive and Negative Syndrome Scale), which includes almost all aspects of the pathology such as depression and anxiety, but with the exception of cognition [13]. Based on the PANSS (but also on other rating scales), there is overwhelming evidence that both FGAs and SGAs significantly reduce the symptoms of schizophrenia. For example, in a recent meta-analysis involving 15 different FGAs and SGAs in a total of more than 43,000 patients [14], all antipsychotics were significantly superior to placebo and there were no differences between individual antipsychotics, with the only exception being clozapine, which was significantly more effective than all the other antipsychotic drugs. This is an interesting finding, as it shows that there are no major differences between FGAs and SGA, at least with respect to the therapeutic effects. This result is consistent with those of several other major multi-center trials [15,16]. A more recent meta-analysis also showed no major differences between haloperidol and 20 other antipsychotic drugs, although only FGAs were included in this study [17].
The PANSS is based on evaluation of both the positive and negative symptoms of schizophrenia; therefore, a reduction in the PANSS score could, in theory, be due to a reduction in either (or both) types of symptoms. However, the available evidence clearly favors a selective improvement in the positive symptoms [18]. Indeed, a larger meta-analysis of 168 independent placebo-controlled trials [19] confirmed that antipsychotics have only a limited effect on the negative symptoms. While the authors found a statistically significant effect of SGAs, the size of the effect (−0.58) was not considered to be clinically relevant. Interestingly, and in support of the previous statement, the size of the effects of FGAs was very similar to that of the SGAs (−0.53) and also statistically significant. Similarly, most studies seem to indicate that antipsychotics have little effect on the cognitive symptoms [20].
A particularly problematic aspect of antipsychotic treatment is the poor compliance of patients with schizophrenia. The CATIE (Clinical Antipsychotic Trials of Intervention Effectiveness) study, a multi-center study involving more than 1,400 patients, was designed primarily to investigate treatment compliance. It revealed that 74% of the patients had discontinued treatment within 18 months (again, with no apparent difference between the antipsychotics prescribed, although olanzapine was associated with slightly better compliance than the other drugs used), with inefficacy and intolerable side-effects cited as the major causes of discontinuation [15]. Although this study was performed in chronic patients, a subsequent study in first episode patients showed very similar discontinuation rates of approximately 70% after 12 months for several SGAs [21]. EUFEST, (European First Episode Schizophrenia Trial), a European multi-center study also conducted in first episode patients, showed substantial discontinuation rates ranging from 33% to 72% within 12 months. Interestingly, in this study, the FGA haloperidol was substantially inferior to the SGAs in terms of discontinuation rates, while symptom reduction was similar for all antipsychotics [16].
Overall then, with respect to therapeutic efficacy, a relatively clear picture has emerged of antipsychotics reducing positive symptoms, but not negative or cognitive symptoms and having relatively high discontinuation rates. Overall, there is little evidence to support the claim that SGAs are superior to FGAs, with the possible exception of clozapine. There is, however, some evidence to suggest that clozapine may be the most effective drug in therapy-resistant patients [10,22]. Although a recent meta-analysis failed to support this superiority for clozapine [23], the authors do point out that this may be due to insufficient statistical power and the fact that sufficient studies with high-dose clozapine, especially in extremely treatment-resistant patients, were lacking from the analysis.
While there appears to be relatively few differences in their therapeutic properties, antipsychotics differ more substantially in their side-effects, with the most important ones being EPS, weight gain, sedation, QTc prolongation and prolactin release (and associated sexual side-effects). As previously mentioned, antipsychotics were traditionally subdivided into “classical” and “atypical” categories based on the idea that classical antipsychotics induce substantially more EPS than atypical drugs. However, recent studies have failed to find support for this distinction. For example the previously mentioned large meta-analysis, which while providing evidence in support of a lack of EPS for clozapine, showed that other so-called atypical antipsychotics (such as risperidone, lurasidone and paliperidone) induced substantial EPS that were not dissimilar to those of typical FGAs (such as chlorpromazine or zotepine) [14]. Furthermore, there were no discernible distinctions between FGAs and SGAs with respect to other side-effects. Thus, while weight gain is a prominent side-effect associated with some SGAs (such as olanzapine, clozapine and iloperidone), it is equally common among FGAs (such as chlorpromazine and zotepine), and virtually absent in several other SGAs (ziprasidone and lurasidone). Overall, the results support the concept that the differences in therapeutic effects between different antipsychotic drugs are relatively small, while the side-effect profiles show more variability, and that the originally proposed distinction between “classical” and “atypical” antipsychotics is not supported by the majority of large-scale clinical studies and meta-analyses.
After the recognition that antipsychotics can substantially reduce the (positive) symptoms of schizophrenia, research (especially in animals) became focused on identifying the underlying neurobiological mechanisms. A landmark paper published in 1963 showed that antipsychotics increased the levels of metabolites of several catecholamines, most notably dopamine and noradrenaline [24]. Three years later, Van Rossum published a paper entitled “The significance of dopamine-receptor blockade for the mechanism of action of neuroleptic drugs” [25]. This study showed that all antipsychotics block the behavioral effects of L-dopa, leading to the formulation of the dopamine hypothesis of antipsychotic drugs. A decade later, two studies revealed a significant linear negative correlation between the average clinical dose of antipsychotics and the affinity for the dopamine D2 receptor [26,27]. However, these studies were performed in vitro and it was only after the development of sensitive radioactive positron emission tomography (PET) ligands for the dopamine D2 receptors that the occupancy of D2 receptors in patients with schizophrenia could be observed directly in vivo [28,29]. These studies revealed that blockade of approximately 60% of the dopamine D2 receptors was necessary to obtain adequate antipsychotic activity, while levels higher than 80% led to the occurrence of EPS [30]. In line with its special clinical profile (see above), clozapine was found to be different from the other antipsychotics in that antipsychotic activity was observed with only 35% D2 receptor blockade. This strongly suggests that additional receptors are involved in the therapeutic actions of clozapine and may provide an explanation for its effectiveness in therapy-resistant patients as wells as the relative lack of EPS. However, the nature of these additional receptor interactions is still unknown. The finding that all antipsychotics (with the possible exception of clozapine) seem to exert their therapeutic effects via blockade of the dopamine D2 receptors, fits in very well with the previously mentioned clinical evidence that there are no substantial differences in the effects of these drugs on positive symptoms. By the same token, the clear differences in binding profiles are more likely to be related to the larger differences in side-effects [11]. For example, blockade of the α1-adrenoceptor has been implicated in cardiovascular side-effects, such as hypotension, while the histamine H1 receptor is involved in sedation and weight gain. Several of the serotonergic receptors, such as the 5-HT2A and 5-HT2C receptors, have been implicated in sexual dysfunction, while the latter, together with the 5-HT1A receptors, have also been implicated in the effects of certain antipsychotics on weight gain.
Bipolar Disorder
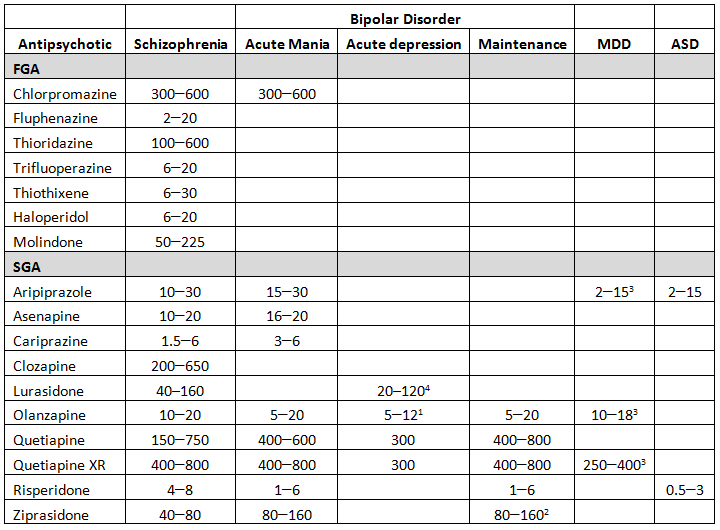
In addition to the treatment of schizophrenia, several antipsychotics have also been approved for the treatment of bipolar disorder (see Table 1). Bipolar disorder comprises a group of several mood-related disorders characterized by periods of depressive and manic symptoms. The most frequently occurring forms are bipolar I (with full blown manic and depressive phases) and bipolar II (with less severe (hypo)manic phases). Cyclothymia refers to a less severe form of bipolar disorder, in which the symptoms of both the manic and the depressive phases are milder than those of bipolar disorder I. Although patients with bipolar disorder suffer from both manic and depressive phases, it is important to realize that the depressive episodes last significantly longer than the manic phases, the ratios being approximately 3:1 for bipolar I and 39:1 for bipolar II [31,32].
Bipolar disorder has a lifetime prevalence of approximately 1% to 2% and is, like schizophrenia, likely to be due to an interaction between genetic and environmental factors [33]. Although the periods of depression are virtually indistinguishable from those seen in major depressive disorders, it is important to know that antidepressants are generally not considered effective treatments for bipolar disorder. Indeed, no antidepressant is currently approved for the treatment of bipolar disorder (at least as a monotherapy) and there is considerable evidence that they can induce a hypomanic phase and/or lead to a phenomenon known as rapid cycling [34]. This is particularly problematic, as many bipolar patients (up to 20%) are misdiagnosed as suffering from a unipolar depression and hence, are treated with standard antidepressant medication [35].
With respect to the treatment of bipolar disorder, a distinction is usually made between acute bipolar mania, acute bipolar depression and bipolar maintenance, with certain antipsychotics being approved for each of the three treatment phases. Given that the manic symptoms resemble the positive symptoms of schizophrenia (especially in relation to delusional thinking), it is not surprising that many antipsychotics have been approved to treat the acute manic phase, including one FGA (chlorpromazine) and multiple SGAs (olanzapine, risperidone, quetiapine, ziprasidone, aripiprazole, asenapine and cariprazine; see Table 1). With the exception of asenapine, these SGAs are also approved for bipolar maintenance therapy. However, there appears to be some important differences among these SGAs, especially with respect to the so-called polarity index (PI) [36], which is an indication of whether a drug is more effective in the treatment of the manic episodes (PI > 1) or the depressive episodes (PI < 1). Whereas nearly all SGAs have a PI above 1 (ranging from 3.9 for olanzapine to 12.1 for risperidone), quetiapine has a PI of 0.8, indicating it is (slightly) more effective in the treatment of depressive episodes.
Table 1 Average doses of antipsychotic drugs for the approved indications (in mg/day) (Abbreviations: MDD: Major Depressive Disorders; ASD: Autism Spectrum Disorder. Footnotes: 1: in combination with fluoxetine; 2: in combination with lithium or valproate; 3: in combination with an antidepressant; 4: alone, or in combination with lithium or valproate).
In accordance with this, quetiapine is the only SGA approved for all three different treatment phases of bipolar disorder, including maintenance and depression phase therapy. Interestingly, until 2003, the United States Food and Drug Administration (FDA) had not approved a single agent for the treatment of bipolar depression. In that year, the combination of the SGA, olanzapine, and the antidepressant, fluoxetine, was approved, followed by two more SGAs (quetiapine in 2006 and lurasidone in 2013). In accordance with these guidelines, the combination of olanzapine and fluoxetine seems superior to olanzapine alone, leading to a shorter onset of action and reduced rate of remission [37,38]. In subsequent studies, quetiapine monotherapy and lurasidone (both as a monotherapy and in combination with either lithium or valproate) were shown to be as effective as the olanzapine/fluoxetine combination [39]. There were, however, some differences with respect to the side-effects. Here, lurasidone (both as a mono- and adjunctive therapy) was superior to the olanzapine/fluoxetine combination (which led to significant weight gain and diarrhea) and quetiapine (which led to significant drowsiness and dry mouth). This is very similar to the differential side-effect profile described previously in patients with schizophrenia [14].
Compared to schizophrenia, much less is known about the neurobiological mechanisms underlying the therapeutic effects of antipsychotics in bipolar disorder. Given the aforementioned similarity between the positive symptoms of schizophrenia and mania, and the fact that virtually all antipsychotics have anti-manic effects, blockade of the dopamine D2 receptor seems to be the most likely mechanism underlying the anti-manic properties of antipsychotics. However, why specific drugs such as quetiapine and lurasidone are also effective in bipolar depression is much less clear. One potential mechanism of action is blockade of 5-HT7 receptors. Both lurasidone and quetiapine have strong 5-HT7 receptor affinities, and animal studies have indicated that 5-HT7 antagonists may have antidepressant activity [40,41]. This may also explain why the average daily dose for treating bipolar depression is considerably lower than that for schizophrenia and mania (see Table 1).
Major Depressive Disorder (MDD)
In contrast to schizophrenia and bipolar disorder, which have a lifetime prevalence of approximately 1%, major depressive disorder (MDD, also referred to as unipolar depression) is much more common, with a lifetime prevalence of around 17% [42]. Patients with major depression disorder (MDD) can display a number of different characteristics, but must include either depressed mood or loss of interest or pleasure in (nearly) all activities. In addition, patients often exhibit altered eating and sleep patterns, psychomotor retardation, lethargy, low self-esteem and recurrent thoughts of death and suicidal ideation. Compared to schizophrenia, MDD develops slightly later in life, with 50% of cases being diagnosed by the age of 32, and is more prevalent in women [42].
Traditionally, MDD is treated with antidepressant drugs, including monoamine oxidase inhibitors, tricyclic antidepressants, selective serotonin reuptake inhibitors and more recently, dual serotonin/noradrenaline reuptake inhibitors. Overall, there is convincing evidence that all these strategies are effective in MDD patients, although only about 33% show full remission [43] and about 50% of patients who do not respond to the first antidepressant are also non-responsive to a second. Even after multiple interventions, approximately 25% of the patients remain depressed and the chances of improvement decrease with the number of failed interventions [44]. Such cases are generally classified as treatment-resistant depression, albeit different definitions exist [45].
Increasingly, atypical antipsychotics are being used as adjunctive therapy for treatment-resistant depression [46]. In the USA, quetiapine, olanzapine and aripriprazole have been approved by the FDA, while in Europe, only quetiapine has been approved [45]. Although all these SGAs have been proven to be effective when administered in combination with antidepressants [47,48,49], their efficacy appears to be limited and most studies have been of short duration (typically 6–8 weeks). In a recent review, the benefits and risks of adjunctive quetiapine (the most commonly used antipsychotic) were evaluated based on data available in the literature [50]. It was concluded that quetiapine did lead to a significant improvement, although the effect was relatively small and again only short-term (6–8 weeks) studies were performed. How long the combined treatment is effective is therefore an important question that remains to be answered. A recent study addressed this issue by randomly assigning 444 treatment-resistant patients to either olanzapine or olanzapine plus fluoxetine (OFC) for up to 47 weeks [51]. Time-to-relapse was significantly longer in the OFC combination group compared to that in the patients treated with olanzapine alone, suggesting a long-term benefit of a combined SGA/antidepressant treatment. Unfortunately, the OFC combination also led to more metabolic side-effects (such as weight gain and increased glucose levels), although extrapyramidal side-effects were similar between the two treatment groups. As a contradiction to this, a recent study suggested that the combination of SGA and antidepressants did not confer any significant benefit as patients given the combination did not score higher in the quality-of-life assessments [52]. However, the authors only used a cross-sectional design, and did not evaluate whether quality-of-life improved during treatment. It was also found that the patients in the combination group scored significantly higher on the personal health questionnaire, indicating that the combination therapy group had a significantly higher incidence of depression, thus making a cross-sectional analysis very difficult.
Overall, the data seem to indicate that the efficacy of adjunctive SGA therapy is not straightforward and may also depend on the patient population. A recent study addressed this issue specifically by reviewing and analyzing the data available in the literature and stratifying the patients based on their resistance to therapy [53]. This analysis clearly showed that the effectiveness of adjunctive SGAs correlated positively with treatment resistance. Thus, while non-treatment-resistant patients did not benefit from adjunctive therapy, patients who were resistant to two or more prior treatments exhibited the largest benefit. Sole baseline depression scores or number of depressive episodes did not predict therapy response, at least for quetiapine [54].
Similar to the situation with bipolar disorder, the neurobiological mechanisms underlying the therapeutic effects of SGAs in treatment-resistant depression are virtually unknown. Moreover, investigations of these mechanisms are further complicated by the fact that SGAs need to be co-administered with standard antidepressant therapies. However, the fact that the doses required to achieve a significant improvement are substantially lower than the antipsychotic dose range for the treatment of schizophrenia (see Table 1), and lack of therapeutic efficacy of most antipsychotics in resistant depression, refutes a major role of the dopamine D2 receptor. Rather, as for the treatment of bipolar depression, a role for serotonergic receptors, such as the 5-HT7 seems more likely.
Autism Spectrum Disorder (ASD)
Autism, or Autism Spectrum Disorder (ASD) as it is called in the Diagnostic and Statistical Manual of Mental Disorders - Fifth Edition (DSM-V), is one of the earliest psychiatric illnesses to occur, with a typical age of onset of 2 to 3 years. Although a number of different subtypes have traditionally been identified, such as true autism (sometimes referred to as low-functioning autism), Asperger syndrome (sometimes referred to as high functioning autism) or atypical autism, the DSM-V no longer differentiates between these subtypes. Patients with ASD have symptoms in three core domains: social interaction, social communication and stereotyped/restrictive behavior and interests. These symptoms typically include deficits in initiating social interaction, abnormal social approach, deficits in non-verbal communications and deficits in developing, maintaining and understanding social relationships. Within the stereotypy domain, repetitive motor movements are often seen, and patients often show insistence on consistency and inflexibility in both behavior and cognitive processes.
The rising incidence of ASD is a cause for concern. Although it is currently debated whether this is a true increase or the result of altered diagnostic criteria and increased awareness or even both, studies in many different countries have reported significant increases over the last two decades. A study in the USA, for instance, found that the incidence of ASD increased from 0.7% in 2000 to 1.5% in 2010 [55], with the incidence in boys being approximately four times higher than that in girls. As a result, the financial burden of ASD is significant, especially since a substantial number of children will continue to show signs of ASD in adulthood. A recent analysis from Great Britain estimated the costs of ASD at £2.7 billion per year for children and over £25 billion for adults [56].
Unfortunately, there are no pharmacological treatments available that affect the core symptoms of ASD. In fact, the only two FDA approved drugs are the SGAs risperidone and aripiprazole. Nevertheless, both are specifically aimed only at reducing irritability and stereotyped behavior. McCracken and colleagues studied the effects of low doses of risperidone (0.5–3.5 mg/day) in children aged 5 to 17 affected by autism and disruptive behavior. In this 8-week study, a significant reduction in aggression, tantrums, irritability and self-injurious behavior was found [57]. Furthermore, such improvements seemed to persist during long-term (6 month) treatment [58]. In addition to risperidone, aripiprazole (FDA approval in 2009) showed a significant improvement in irritability and overall quality-of-life. In a recent meta-analysis, aripiprazole was found to lead to significant improvements in irritability and hyperactivity [59]. Several other antipsychotics such has haloperidol, clozapine and ziprasidone have been evaluated in patients with ASD, although these drugs showed either a smaller therapeutic effect or substantial side-effects [60,61].
Inspection of Table 1 shows that the dose for treating ASD is relatively low, certainly when compared to the doses administered for the treatment of schizophrenia and mania. This may in part be due to differences in the pharmacokinetic characteristics of the drug between children and adults, but may also indicate a different underlying mechanism of action. The neurochemical basis of autism is still largely unknown, yet some studies have implicated abnormal dopaminergic and especially serotoninergic transmission as a pathological factor [62]. These two neurotransmitter systems are modulated by antipsychotics including risperidone and aripiprazole, as we have discussed previously.
Off-Label Use of Antipsychotics
Like many other drugs, antipsychotics are used not only for approved indications, but also in an off-label approach. This includes the use of non-approved antipsychotics for the indications we discussed previously (haloperidol for the treatment of mania or ASD, and aripiprazole for the treatment of bipolar depression [63,64]), as well as the use of antipsychotics for other indications, such as generalized anxiety disorder, attention-deficit hyperactivity disorder (ADHD), anorexia nervosa, dementia and other conditions. Off-label use is widespread among antipsychotics and studies have shown that SGAs are used for off-label treatment of psychiatric disorders more than any other type of psychotropic medication [65]. Moreover, off-label use of antipsychotics is on the increase, from 4.4 million treatment-related visits in 1995 to 9 million in 2008, leading to a total off-label cost of 6 billion in 2008. Importantly, these studies also estimated that 90% of the use was for indications for which there was no compelling evidence of benefit [66].
A recent study in the UK confirmed the extensive use of antipsychotics for non-approved indications [67]. In this study, data from almost 48,000 patients were collected from The Health Improvement Network (THIN), a primary care database of routine clinical care and administration information. The results showed that haloperidol, chlorpromazine and trifluoperazine were the three most commonly prescribed FGAs and olanzapine, risperidone and quetiapine were the most commonly prescribed SGAs. In accordance with the previously mentioned study from the US [66], the minority of patients that were prescribed antipsychotics suffered from schizophrenia, bipolar disorder or another disorder for which antipsychotics are approved. As Figure 3 clearly shows, the only exception was olanzapine. Most of the other antipsychotics were prescribed for depression and anxiety disorder, and a significant proportion (especially in the case of haloperidol) also for dementia. Although there is some evidence that aripiprazole and risperidone improve psychiatric symptoms in patients with dementia (especially in relation to aggression and psychosis), these drugs also induce substantial side-effects (especially sleep disturbance, Parkinsonism, pneumonia, stroke and urinary infections) [68]. Moreover, a recent study convincingly showed a significant relationship between the dose of antipsychotic drug used and mortality in elderly patients [69]. Taken together, these findings indicate that the use of antipsychotics in elderly patients should not be promoted.
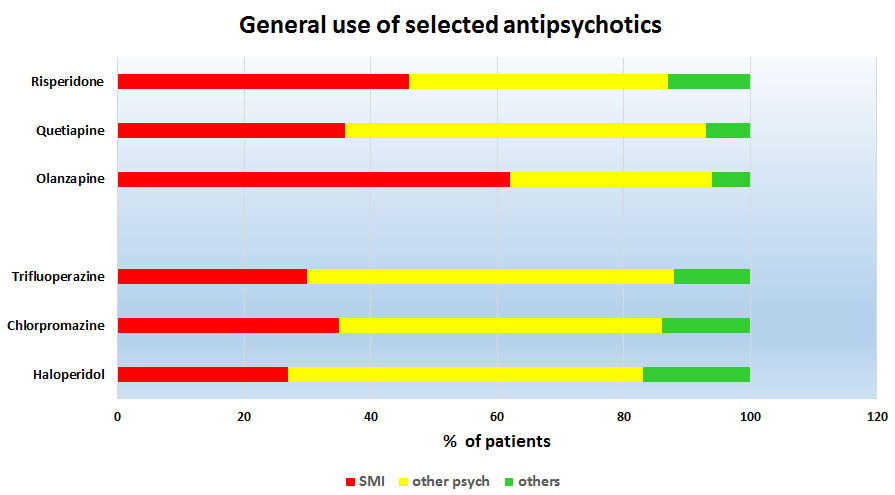
Figure 3 The use of the three most commonly prescribed second-generation antipsychotics (SGAs, top) and first-generation antipsychotics (FGAs, bottom) for serious mental illness (SMI, approved indication), other psychiatric disorders (other psych; such as mood disorders, anxiety disorders and dementia) and other disorders.
In addition to the rise in use of antipsychotics in the elderly population, there is also evidence of increased prescription for children. In the UK, the use of antipsychotic medication in children under 18 doubled between 1994 and 2005 (from 0.4 to 0.8 per 1,000 patient years), with the largest increase in the 7- to 12-year-old age group [70]. In the US, a 22% increase in antipsychotic use was registered between 2004 and 2008, although a decline was seen between 2008 and 2010 [71]. This increase is a major concern for several reasons. First of all, antipsychotics were developed for the treatment of adults, not adolescents or children. Perhaps more importantly, in young children, the brain is still developing rapidly [72,73] and drugs may therefore, have very different and perhaps, longer-lasting effects. This is especially likely for antipsychotic drugs, as they influence neurotransmitters such as dopamine and serotonin that have neurotrophic effects in the developing brain. Serotonin, for instance, influences synaptogenesis, axonal guidance, and neurite outgrowth as well as other developmental processes [74]. Therefore, although prescribing drugs always involves an evaluation of the risks and benefits, in the case of antipsychotics prescribed for children, this issue becomes even more pertinent.
To assess the effectiveness of antipsychotic treatments in children, a detailed analysis of the pattern of prescription is necessary. As discussed previously, in relation to childhood psychiatric disorders, only risperidone and aripiprazole are indicated for the treatment of ASD, and these drugs have been shown to be effective. Smaller scale studies with other SGAs, such as olanzapine and ziprasidone, and even with the FGA haloperidol, have shown that most of these drugs are effective against agitation/irritability and stereotypy [75]. Both bipolar disorder and schizophrenia typically occur after puberty; however, there is evidence for the occurrence of childhood onset forms of both disorders. The incidence of early-onset bipolar disorder was about 0.24% in 2005 and 0.26% in 2007, with 25% of these children treated before the age of 13. Many (approximately 40%) were prescribed an antipsychotic/mood stabilizer combination [76]. A recent meta-analysis of pharmacological treatment of pediatric bipolar disorder found a significant positive effect of antipsychotics [77] and although antipsychotics are not indicated for preschool children (aged < 6), risperidone, olanzapine and quetiapine were found to be effective in this age group [78,79].
Antipsychotic drugs are also being prescribed for behavioral disorders, attention deficit disorder and Tourette syndrome, although the evidence that they are effective in these disturbances is far from convincing. Given that some of the side-effects are more pronounced in young children than in adults (for instance weight gain [80] and metabolic disturbances [81]), and that there is the aforementioned risk of long-term neurodevelopmental changes (which may not become apparent until much later), the use of antipsychotics for children presents a challenge for both families and physicians. As was recently concluded in a review: “Pragmatism in clinical practice, mindful of the limited evidence base that does exist and the propensity for harm, is necessary; far more research is required in this important area” [75].
Conclusions
About 65 years ago, two French psychiatrists began administering chlorpromazine in an attempt to improve the condition of patients with schizophrenia, thereby triggering an unprecedented revolution in psychopharmacology and psychiatry. Since then, more than 50 different antipsychotics have been developed and they remain the drugs of choice for the treatment of schizophrenia. The re-introduction of clozapine heralded the age of the SGA. Initially, these drugs appeared to be more effective in the treatment of negative and cognitive symptoms; however, this original promise was not substantiated by most large-scale studies and meta-analysis. Nevertheless, most of these drugs do induce fewer EPS and some have also been found to improve other mental conditions, such as bipolar disorder, treatment-resistant depression and ASD. In addition, antipsychotic drugs are increasingly prescribed for indications other than those that are officially approved, including prescription in vulnerable patient groups such as young children and elderly patients (especially those with dementia). Current research does not allow a firm conclusion about the usefulness of these drugs in such conditions and hence, more systematic research is certainly needed to make a proper evaluation of the benefits and risks of the use of antipsychotic drugs in these circumstances.
Many questions around the mechanism(s) of action of antipsychotic drugs remain despite a tremendous amount of research. While it seems generally accepted that the antipsychotic effect (i.e., the reduction in psychotic (positive) symptoms in schizophrenia and bipolar mania) are mediated via blockade of dopamine D2 receptors, it is less clear why certain SGAs are beneficial in the treatment of depressive symptoms (in bipolar and MDDs). Similarly, while it is generally recognized that clozapine has a unique profile and is effective in treatment-resistant patients with schizophrenia, it is, as yet, unclear through which neurobiological mechanism this is mediated. The fact that, in contrast to other antipsychotics, clozapine blocks only about 35% of dopamine D2 receptors, clearly points to the involvement of other receptors. In fact, antipsychotics possess a “promiscuous” affinity for different neurotransmitters receptors, a profile of binding that varies with each drug and that might be one cause of the somewhat clinically inconsistent responses reported in the literature.
In summary, antipsychotics have had a major positive influence on patients with severe mental disorders, and continue to play a major role in their treatment. However, there are still important limitations that need to be addressed. For example, the lack of effect on negative and cognitive symptoms in schizophrenia remains a major shortcoming, and it is still unclear how effective SGAs are in the long-term therapy of treatment-resistant depression. Finally, one of the major limitations is poor patient compliance, especially in schizophrenia, given that continued treatment is the most important factor in preventing relapse. Together with improving the therapeutic efficacy, a reduction in adverse side-effects (such as EPS and weight gain) would contribute considerably to enhancing the therapeutic potential of antipsychotic drugs. A greater understanding of the neurobiology of these drugs is paramount for achieving these objectives.
Future Directions
This review clearly emphasizes the enormous influence antipsychotics have had on the course and outcome of schizophrenia, and also, in more recent years, the contribution they have made for the treatment of other psychiatric disorders, such as BP, MDD and ASD. However, the treatment of these disorders is far from perfect. The relatively low patient compliance rates, the lack of effect of antipsychotics on the negative and cognitive symptoms in schizophrenia and on the core symptoms of ASD are important limitations. Moreover, from a mechanistic point of view, the mechanism of action of clozapine (which appears to be unique among the SGAs) and the neurobiological substrate underlying the therapeutic effects of SGAs in BP, MDD and ASD are still largely unknown. An improved understanding would improve our chances of developing more effective treatments.
A detailed outline of the development of novel treatments for the disorders discussed is beyond the scope of this review. Suffice it to say that several different strategies are currently being pursued. On one hand, we have “more of the same” type strategies, in which proven neurobiological mechanisms are further optimized. For schizophrenia, for example, this would include more specific dopamine antagonists or dopamine/serotonin dual antagonists [11], while for major depression, selective inhibitors of all three monoamine transporters (serotonin, noradrenaline and dopamine) are being developed [82]. On the other hand, we have novel therapeutic mechanisms that, so far, have shown limited success. In schizophrenia, drugs based on enhancing glutamate neurotransmission have long been thought to be promising alternatives to antipsychotic drugs. However, the recent failures of drugs interacting with the glutamate transporter [83], or with the metabotropic glutamate receptors [84,85], have tempered our hopes substantially. For the treatment of MDD, however, glutamatergic therapies (based on the clinical effectiveness of ketamine, an NMDA receptor antagonist) are still considered to be potentially useful [82]. Similarly, ketamine is being considered as an add-on therapy for BP [86]. Interventions aimed at altering the cholinergic system are also being pursued, both for schizophrenia [87], and MDD [88].
However, technically-speaking, these drugs are not likely to be effective antipsychotics, as most evidence suggests that they are more effective in the treatment of negative and cognitive symptoms than in reducing psychotic (positive) symptoms, and indeed, most have been combined with a standard antipsychotic drug [89–91]. Nonetheless, it is hoped that these, and potentially other treatments, will substantially improve the course and outcome of patients with severe psychiatric disorders.
Author Contributions
All authors contributed to the ideas and the writing presented in this review.
Competing Interests
The authors have declared that no competing interests exist.
References
- Moncrieff J. Magic bullets for mental disorders: the emergence of the concept of an 'antipsychotic' drug. J Hist Neurosci. 2013;22(1):30-46. [CrossRef]
- Laborit H, Huguenard P, Alluaume R. [A new vegetative stabilizer; 4560 R.P..]. Presse Med. 1952;60(10):206-8.
- Laborit H, Huguenard P. [Artificial hibernation by pharmacodynamical and physical means]. Presse Med. 1951;59(64):1329.
- Delay J, Deniker P, Harl JM. Therapeutic use in psychiatry of phenothiazine of central elective action (4560 RP). Ann Med Psychol (Paris). 1952;110(2:1):112-7.
- Guttmacher MS. Phenothiazine Treatment in Acute Schizophrenia; Effectiveness: The National Institute of Mental Health Psychopharmacology Service Center Collaborative Study Group. Arch Gen Psychiatry. 1964;10:246-61.
- Haase HJ. About Prevalence and Interpretation of the psychomotor Parkinson Syndrome in Megaphen or Largactil Treatment Duration. Nervenarzt. 1954;25(12):486-92.
- Steck H. Le syndrome extra-pyramidal et di-encephalique au cours des traitments au Largactil et au Serpasil. Ann Med Psychol. 1954;112:737-43.
- Haase HJ, Zahn M, Zschucke CF. Influence of Anti-Neuroleptic Action on the Neuroceptic Threshold. Int J Neuropsychiatry. 1965;1(3):239-52.
- Idanpaan-Hiekkila J, Alhave E, Olkinuora M, Plava I. Agranulocytosis during treatment with clozapine. Eur J Clin Pharmacol. 1977;11:193-8. [CrossRef]
- Kane JM, Honigfeld G, Singer J, Meltzer HY. Clozapine for the treatment-resistant schizophrenic: A double-blind comparison with chlorpromazine. Arch Gen Psychiatry. 1988;45:789-96. [CrossRef]
- Ellenbroek BA, Cesura AM. Antipsychotics and the dopamine-serotonin connection. In: Celanire S, Poli S, editors. Topics in Medicinal Chemistry. 13. Heidelberg: Springer; 2015. p. 1-50.
- Hafner H, Maurer K, Loffler W, Riecher RA. The influence of age and sex on the onset and early course of schizophrenia. Br J Psychiatry. 1993;162(1):80-6. [CrossRef]
- Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261-76. [CrossRef]
- Leucht S, Cipriani A, Spineli L, Mavridis D, Orey D, Richter F, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382(9896):951-62. [CrossRef]
- Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-23. [CrossRef]
- Kahn RS, Fleischhacker WW, Boter H, Davidson M, Vergouwe Y, Keet IP, et al. Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trial. Lancet. 2008;371(9618):1085-97. [CrossRef]
- Dold M, Tardy M, Samara MT, Li CB, Kasper S, Leucht S. Are all first-generation antipsychotics equally effective in treating schizophrenia? A meta-analysis of randomised, haloperidol-controlled trials. World J Biol Psychiatry. 2016;17(3):210-20. [CrossRef]
- Salimi K, Jarskog LF, Lieberman JA. Antipsychotic drugs for first-episode schizophrenia: a comparative review. CNS Drugs. 2009;23(10):837-55. [CrossRef]
- Fusar-Poli P, Papanastasiou E, Stahl D, Rocchetti M, Carpenter W, Shergill S, et al. Treatments of Negative Symptoms in Schizophrenia: Meta-Analysis of 168 Randomized Placebo-Controlled Trials. Schizophr Bull. 2015;41(4):892-9. [CrossRef]
- Keefe RSE, Bilder RM, Davis SM, Harvey PD, Palmer BW, Gold JM, et al. Neurocognitive effects of antipsychotic medications in patients with chronic schizophrenia in the CATIE trial. Arch Gen Psychiatry. 2007;64(6):633-47. [CrossRef]
- McEvoy JP, Lieberman JA, Perkins DO, Hamer RM, Gu H, Lazarus A, et al. Efficacy and tolerability of olanzapine, quetiapine, and risperidone in the treatment of early psychosis: A randomized, double-blind 52-week comparison. Am J Psychiatry. 2007;164:1050-60. [CrossRef]
- McEvoy JP, Lieberman JA, Stroup TS, Davis SM, Meltzer HY, Rosenheck RA, et al. Effectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior atypical antipsychotic treatment. Am J Psychiatry. 2006;163(4):600-10. [CrossRef]
- Samara MT, Dold M, Gianatsi M, Nikolakopoulou A, Helfer B, Salanti G, et al. Efficacy, Acceptability, and Tolerability of Antipsychotics in Treatment-Resistant Schizophrenia A Network Meta-analysis. JAMA Psychiatry. 2016;73(3):199-210. [CrossRef]
- Carlsson A, Lindqvist M. Effects of chlorpromazine or haloperidol on formation of 3-methoxytyramin and normetanephrine in mouse brain. Acta Pharmacol Toxicol. 1963;20:140-4. [CrossRef]
- van Rossum J. The significance of dopamine-receptor blockade for the mechanism of action of neuroleptic drugs. Arch Int Pharmacodyn Ther. 1966;160(2):492-4.
- Seeman P, Lee T, Choa-Wong M, Wong K. Antipsychotic drug doses and neuroleptic/dopamine receptors. Nature. 1976;261:717-9. [CrossRef]
- Creese I, Burt D, Snyder SH. Dopamine receptor binding predicts clinical and pharmacological potenties of antischizophrenic drugs. Science. 1976;192:481-3. [CrossRef]
- Farde L, Wiesel FA, Nordstrom AL, Sedvall G. D1 and D2 dopamine receptor occupancy during treatment with conventional and atypical neuroleptics. Psychopharmacology. 1989;99:S28-S31. [CrossRef]
- Farde L, Wiesel FA, Halldin C, Sedvall G. Central D2-dopamine receptor occupancy in schizophrenic patients treated with antipsychotic drugs. Arch Gen Psychiatry. 1988;45(1):71-6. [CrossRef]
- Nord M, Farde L. Antipsychotic occupancy of dopamine receptors in schizophrenia. CNS Neurosci Ther. 2011;17(2):97-103. [CrossRef]
- Judd LL, Akiskal HS, Schettler PJ, Coryell W, Endicott J, Maser JD, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry. 2003;60(3):261-9. [CrossRef]
- Judd LL, Akiskal HS, Schettler PJ, Endicott J, Maser J, Solomon DA, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry. 2002;59(6):530-7. [CrossRef]
- Ellenbroek BA, Youn J. Affective Disorders. Gene-Environment Interactions in psychiatry Nature, nurture, neuroscience. London: Elsevier; 2016.
- Pacchiarotti I, Bond DJ, Baldessarini RJ, Nolen WA, Grunze H, Licht RW, et al. The International Society for Bipolar Disorders (ISBD) task force report on antidepressant use in bipolar disorders. Am J Psychiatry. 2013;170(11):1249-62. [CrossRef]
- Hirschfeld RM, Cass AR, Holt DC, Carlson CA. Screening for bipolar disorder in patients treated for depression in a family medicine clinic. J Am Board Fam Pract. 2005;18(4):233-9. [CrossRef]
- Popovic D, Reinares M, Goikolea JM, Bonnin CM, Gonzalez-Pinto A, Vieta E. Polarity index of pharmacological agents used for maintenance treatment of bipolar disorder. Eur Neuropsychopharmacol. 2012;22(5):339-46. [CrossRef]
- Tohen M, Vieta E, Calabrese J, Ketter TA, Sachs G, Bowden C, et al. Efficacy of olanzapine and olanzapine-fluoxetine combination in the treatment of bipolar I depression. Arch Gen Psychiatry. 2003;60(11):1079-88. [CrossRef]
- McIntyre RS, Cha DS, Kim RD, Mansur RB. A review of FDA-approved treatment options in bipolar depression. CNS Spectr. 2013;18 Suppl 1:4-20; quiz 1. [CrossRef]
- Citrome L. Treatment of bipolar depression: making sensible decisions. CNS Spectr. 2014;19 Suppl 1:4-11; quiz 1-3, 2.
- Gellynck E, Heyninck K, Andressen KW, Haegeman G, Levy FO, Vanhoenacker P, et al. The serotonin 5-HT7 receptors: two decades of research. Exp Brain Res. 2013;230(4):555-68. [CrossRef]
- Naumenko VS, Popova NK, Lacivita E, Leopoldo M, Ponimaskin EG. Interplay between serotonin 5-HT1A and 5-HT7 receptors in depressive disorders. CNS Neurosci Ther. 2014;20(7):582-90. [CrossRef]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602. [CrossRef]
- Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry. 2006;163(1):28-40. [CrossRef]
- Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163(11):1905-17. [CrossRef]
- Kasper S. Treatment-resistant depression: a challenge for future research. Acta Neuropsychiatr. 2014;26(3):131-3. [CrossRef]
- Gerhard T, Akincigil A, Correll CU, Foglio NJ, Crystal S, Olfson M. National Trends in Second-Generation Antipsychotic Augmentation for Nonpsychotic Depression. J Clin Psychiatry. 2014;75(5):490-7. [CrossRef]
- Connolly KR, Thase ME. Emerging drugs for major depressive disorder. Expert Opin Emerg Drugs. 2012;17(1):105-26. [CrossRef]
- Han C, Wang SM, Kato M, Lee SJ, Patkar AA, Masand PS, et al. Second-generation antipsychotics in the treatment of major depressive disorder: current evidence. Expert Rev Neurother. 2013;13(7):851-70. [CrossRef]
- Zhou X, Keitner GI, Qin B, Ravindran AV, Bauer M, Del Giovane C, et al. Atypical Antipsychotic Augmentation for Treatment-Resistant Depression: A Systematic Review and Network Meta-Analysis. Int J Neuropsychopharmacol. 2015;18(11):pyv060. [CrossRef]
- Pringsheim T, Gardner D, Patten SB. Adjunctive treatment with quetiapine for major depressive disorder: are the benefits of treatment worth the risks? BMJ. 2015;350:h569. [CrossRef]
- Brunner E, Tohen M, Osuntokun O, Landry J, Thase ME. Efficacy and Safety of Olanzapine/Fluoxetine Combination vs Fluoxetine Monotherapy Following Successful Combination Therapy of Treatment-Resistant Major Depressive Disorder. Neuropsychopharmacology. 2014;39(11):2549-59. [CrossRef]
- Al-Ruthia YS, Hong SH, Solomon D. Do depressed patients on adjunctive atypical antipsychotics demonstrate a better quality of life compared to those on antidepressants only? A comparative cross-sectional study of a nationally representative sample of the US population. Res Social Adm Pharm. 2015;11(2):228-40. [CrossRef]
- Wang HR, Woo YS, Ahn HS, Ahn IM, Kim HJ, Bahk WM. Can Atypical Antipsychotic Augmentation Reduce Subsequent Treatment Failure More Effectively Among Depressed Patients with a Higher Degree of Treatment Resistance? A Meta-Analysis of Randomized Controlled Trials. Int J Neuropsychopharmacol. 2015;18(8):pyv023. [CrossRef]
- Bauer M, Thase ME, Liu S, Earley W, Eriksson H. Analysis of potentially predictive factors of efficacy of adjunct extended-release quetiapine fumarate in patients with major depressive disorder. J Psychopharmacol. 2015;29(5):565-74. [CrossRef]
- Wingate M, Kirby RS, Pettygrove S, Cunniff C, Schulz E, Ghosh T, et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2010. Mmwr Surveillance Summaries. 2014;63(2).
- Knapp M, Romeo R, Beecham J. Economic cost of autism in the UK. Autism. 2009;13(3):317-36. [CrossRef]
- McCracken JT, McGough J, Shah B, Cronin P, Hong D, Aman MG, et al. Risperidone in children with autism and serious behavioral problems. N Engl J Med. 2002;347(5):314-21. [CrossRef]
- Williams SK, Scahill L, Vitiello B, Aman MG, Arnold LE, McDougle CJ, et al. Risperidone and adaptive behavior in children with autism. J Am Acad Child Adolesc Psychiatry. 2006;45(4):431-9. [CrossRef]
- Ching H, Pringsheim T. Aripiprazole for autism spectrum disorders (ASD). The Cochrane database of systematic reviews. 2012;5:CD009043. [CrossRef]
- LeClerc S, Easley D. Pharmacological therapies for autism spectrum disorder: a review. P T. 2015;40(6):389-97.
- Dominick K, Wink LK, McDougle CJ, Erickson CA. A Retrospective Naturalistic Study of Ziprasidone for Irritability in Youth with Autism Spectrum Disorder. J Child Adolesc Psychopharmacol. 2015;25(5):397-401. [CrossRef]
- Lam KS, Aman MG, Arnold LE. Neurochemical correlates of autistic disorder: a review of the literature. Res dev disabil. 2006;27(3):254-89. [CrossRef]
- Yildiz A, Vieta E, Leucht S, Baldessarini RJ. Efficacy of antimanic treatments: meta-analysis of randomized, controlled trials. Neuropsychopharmacology. 2011;36(2):375-89. [CrossRef]
- Cruz N, Sanchez-Moreno J, Torres F, Goikolea JM, Valenti M, Vieta E. Efficacy of modern antipsychotics in placebo-controlled trials in bipolar depression: a meta-analysis. Int J Neuropsychopharmacol. 2010;13(1):5-14. [CrossRef]
- Schutte-Rodin S, Broch L, Buysse D, Dorsey C, Sateia M. Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med. 2008;4(5):487-504.
- Alexander GC, Gallagher SA, Mascola A, Moloney RM, Stafford RS. Increasing off-label use of antipsychotic medications in the United States, 1995-2008. Pharmacoepidemiol Drug Saf. 2011;20(2):177-84. [CrossRef]
- Marston L, Nazareth I, Petersen I, Walters K, Osborn DPJ. Prescribing of antipsychotics in UK primary care: a cohort study. BMJ Open. 2014;4(12):e006135. [CrossRef]
- Tan L, Tan L, Wang HF, Wang J, Tan CC, Tan MS, et al. Efficacy and safety of atypical antipsychotic drug treatment for dementia: a systematic review and meta-analysis. Alzheimers Res Ther. 2015;7(1):20. [CrossRef]
- Gerhard T, Huybrechts K, Olfson M, Schneeweiss S, Bobo WV, Doraiswamy PM, et al. Comparative mortality risks of antipsychotic medications in community-dwelling older adults. Br J Psychiatry. 2014;205(1):44-51. [CrossRef]
- Rani F, Murray ML, Byrne PJ, Wong ICK. Epidemiologic features of antipsychotic prescribing to children and adolescents in primary care in the United Kingdom. Pediatrics. 2008;121(5):1002-9. [CrossRef]
- Olfson M, King M, Schoenbaum M. Treatment of Young People With Antipsychotic Medications in the United States. Jama Psychiatry. 2015;72(9):867-74. [CrossRef]
- Paus T, Keshavan M, Giedd JN. Why do many psychiatric disorders emerge during adolescence? Nat Rev Neurosci. 2008;9(12):947-57. [CrossRef]
- Semple BD, Blomgren K, Gimlin K, Ferriero DM, Noble-Haeusslein LJ. Brain development in rodents and humans: Identifying benchmarks of maturation and vulnerability to injury across species. Prog Neurobiol. 2013;106-107:1-16. [CrossRef]
- Gaspar P, Cases O, Maroteaux L. The developmental role of serotonin: news from mouse molecular genetics. Nature reviews Neuroscience. 2003;4(12):1002-12. [CrossRef]
- Memarzia J, Tracy D, Giaroli G. The use of antipsychotics in preschoolers: A veto or a sensible last option? J Psychopharmacol. 2014;28(4):303-19. [CrossRef]
- Dusetzina SB, Weinberger M, Gaynes BN, Farley JF, Sleath B, Hansen RA. Prevalence of Bipolar Disorder Diagnoses and Psychotropic Drug Therapy Among Privately Insured Children and Adolescents. Pharmacotherapy. 2012;32(12):1085-94. [CrossRef]
- Liu HY, Potter MP, Woodworth KY, Yorks DM, Petty CR, Wozniak JR, et al. Pharmacologic Treatments for Pediatric Bipolar Disorder: A Review and Meta-Analysis. J Am Acad Child Adolesc Psychiatry. 2011;50(8):749-62. [CrossRef]
- Biederman J, Mick E, Hammerness P, Harpold T, Aleardi M, Dougherty M, et al. Open-label, 8-week trial of olanzapine and risperidone for the treatment of bipolar disorder in preschool-age children. Biol Psychiatry. 2005;58(7):589-94. [CrossRef]
- Joshi G, Petty C, Wozniak J, Faraone SV, Doyle R, Georgiopoulos A, et al. A prospective open-label trial of quetiapine monotherapy in preschool and school age children with bipolar spectrum disorder. J Affect Disord. 2012;136(3):1143-53. [CrossRef]
- Safer DJ. Age-Grouped Differences in Adverse Drug Events from Psychotropic Medication. J Child Adolesc Psychopharmacol. 2011;21(4):299-309. [CrossRef]
- De Hert M, Dobbelaere M, Sheridan EM, Cohen D, Correll CU. Metabolic and endocrine adverse effects of second-generation antipsychotics in children and adolescents: A systematic review of randomized, placebo controlled trials and guidelines for clinical practice. Eur Psychiatry. 2011;26(3):144-58. [CrossRef]
- Dale E, Bang-Andersen B, Sanchez C. Emerging mechanisms and treatments for depression beyond SSRIs and SNRIs. Biochem Pharmacol. 2015;95(2):81-97. [CrossRef]
- Bugarski-Kirola D, Wang A, Abi-Saab D, Blattler T. A phase II/III trial of bitopertin monotherapy compared with placebo in patients with an acute exacerbation of schizophrenia - Results from the CandleLyte study. Eur Neuropsychopharmacol. 2014;24(7):1024-36. [CrossRef]
- Cook D, Brown D, Alexander R, March R, Morgan P, Satterthwaite G, et al. Lessons learned from the fate of AstraZeneca's drug pipeline: a five-dimensional framework. Nat Rev Drug Discov. 2014;13(6):419-31. [CrossRef]
- Kinon BJ, Millen BA, Zhang L, McKinzie DL. Exploratory analysis for a targeted patient population responsive to the metabotropic glutamate 2/3 receptor agonist pomaglumetad methionil in schizophrenia. Biol Psychiatry. 2015;78(11):754-62. [CrossRef]
- Data-Franco J, Singh A, Popovic D, Ashton M, Berk M, Vieta E, et al. Beyond the therapeutic shackles of the monoamines: New mechanisms in bipolar disorder biology. Prog Neuropsychopharmacol Biol Psychiatry. 2017;72:73-86. [CrossRef]
- Rowe AR, Mercer L, Casetti V, Sendt KV, Giaroli G, Shergill SS, et al. Dementia praecox redux: A systematic review of the nicotinic receptor as a target for cognitive symptoms of schizophrenia. J Psychopharmacol. 2015;29(2):197-211. [CrossRef]
- O'Leary OF, Dinan TG, Cryan JF. Faster, better, stronger: towards new antidepressant therapeutic strategies. Eur J Pharmacol. 2015;753:32-50. [CrossRef]
- Haig GM, Bain EE, Robieson WZ, Baker JD, Othman AA. A Randomized Trial to Assess the Efficacy and Safety of ABT-126, a Selective alpha 7 Nicotinic Acetylcholine Receptor Agonist, in the Treatment of Cognitive Impairment in Schizophrenia. Am J Psychiatry. 2016;173(8):827-35. [CrossRef]
- Umbricht D, Keefe RSE, Murray S, Lowe DA, Porter R, Garibaldi G, et al. A Randomized, Placebo-Controlled Study Investigating the Nicotinic alpha 7 Agonist, RG3487, for Cognitive Deficits in Schizophrenia. Neuropsychopharmacology. 2014;39(7):1568-77. [CrossRef]
- Lieberman JA, Dunbar G, Segreti AC, Girgis RR, Seoane F, Beaver JS, et al. A randomized exploratory trial of an alpha-7 nicotinic receptor agonist (TC-5619) for cognitive enhancement in schizophrenia. Neuropsychopharmacology. 2013;38(6):968-75. [CrossRef]

